



Abstract:
Since November 2015, at least 10 states in Nigeria have been affected by an outbreak of Lassa fever, an acute viral disease that causes fever, muscle pain, hemorrhage and sometimes death. Of the cases reported so far in the Nigerian outbreak, the mortality rate is 43.2%5 although the typical mortality rate is thought to be closer to 1-15%6. Lassa fever is spread through direct contact with the urine and droppings of the Mastomys natalensis, or ‘multimammate rat’, as well as through contact with the blood, tissue or secretions of a person infected with the Lassa fever virus.
Main Article:
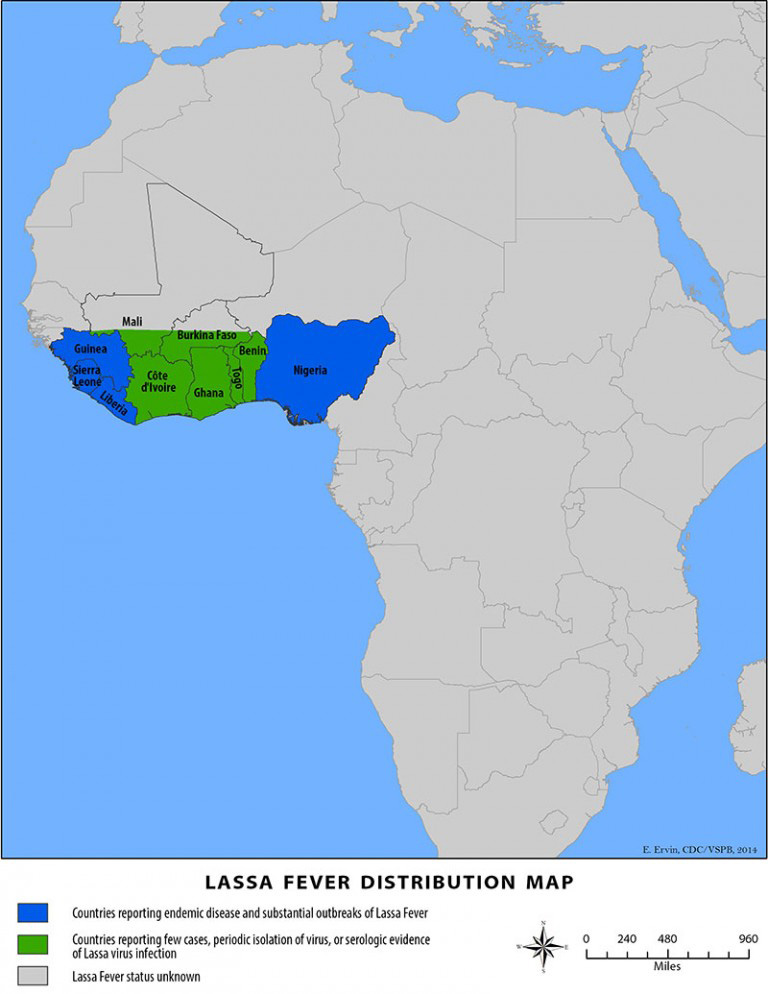
Lassa fever virus was first identified in 1969 in Nigeria. The virus is a member of the Arenaviridae virus family and is a single-stranded RNA, zoonotic virus. The animal vector for the disease is the multimammate rat, which can be found throughout sub-Saharan Africa, except for the south-western portion of the continent. Despite the prevalence of the rat in Africa, Lassa fever is so far only endemic in parts of west Africa, including Nigeria, Liberia, Guinea and Sierra Leone. In some areas of Sierra Leone and Liberia, 10-16% of people admitted to hospitals every year are infected with Lassa fever.1
Transmission:
Lassa fever is spread through direct contact with the urine and droppings of the Mastomys natalensis, or ‘multimammate rat’, as well as through contact with the blood, tissue or secretions of a person infected with the Lassa fever virus. Poor infection prevention and control measures in healthcare settings have also been identified as risk factors for transmission.
Symptoms and Complications
About 80% of people infected with Lassa fever virus infections never develop symptoms. The incubation period between infection and symptoms is between 6 and 21 days. Symptoms present gradually and may include:
- fever
- weakness
- headache
- sore throat
- nausea
- bleeding from mouth, nose, vagina or gastrointestinal tract
- low blood pressure
Hearing loss, sometimes permanent, is the most common complication of Lassa fever. Death occurs in only 1% of all Lassa fever virus infections, but 15-20% of patients infected with Lassa are hospitalized for the disease. The death rates for pregnant women in their third trimester are notably high.
Treatment
The most common treatment for Lassa fever is Ribavirin, which is an antiviral drug. It is most effective when administered early in the course of the illness. Patients should also receive fluids and treatment for blood pressure and other complicating infections.
Prevention
To prevent transmission of Lassa virus from the multimammate rat, Africans in the outbreak regions are encouraged to prevent the rodents from entering the home through improved house maintenance and preventing transmission to food sources by covering food and cleaning preparation, cooking and eating surfaces. Grains (cereals/legumes and other foods in granular form) and other foodstuffs should be stored in rodent-proof containers and garbage disposal should be far from the home. Cats are also helpful for rodent control. Rodents should not be used as a food source.
Healthcare workers and caregivers should observe the following precautions when caring for an infected patient:
- Wear protective clothing, including gloves, goggles, masks and gowns
- Use only sterilized equipment
- Isolate the patient from contact with unprotected persons until the disease has run its course
Recent Lassa Fever Outbreak in Nigeria
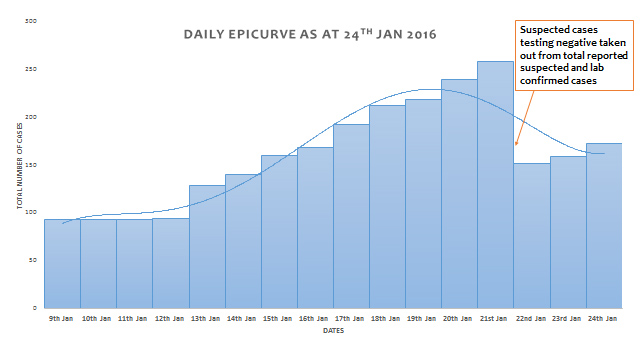
In Nigeria, the Lassa fever virus reached its peak in 2012 with 1,723 cases and 112 deaths and has been declining since then.5 The latest outbreak, believed to have started in November 2015, has so far reported 172 cases with 83 deaths (48%). Ten (10) of the 36 states of the nation were initially affected and include: Bauchi, Nassarawa, Niger, Taraba, Kano, Rivers, Edo, Plateau, Gombe and Oyo States5. As of January 24, 2016, 18 states are currently following up contacts or have suspected cases with laboratory results pending or laboratory confirmed cases4. Response to the outbreak has been prompt, led by the Minister of Health for Nigeria, Professor Isaac Folorunsho Adewole, who has initiated the following measures to control the outbreak:
- Authorized immediate release of adequate quantities of Ribavirin (the specific antiviral drug for Lassa fever) to all the affected states.
- Ordered deployment of rapid response teams to all the affected states to assist in investigating and verifying the cases, as well as tracing of contacts.
- Mobilized and trained clinicians and relevant healthcare workers in areas of patient management and care in the affected states.
- Promoted awareness campaigns across the nation on the signs and symptoms including preventive measures, including fumigation of public places, such as markets, to rid them of rodents and consequently the vector (multimammate rat).
According to Professor Adewole, what is particularly disturbing about the current outbreak is the unusually high number of deaths compared to previous outbreaks. Food storage and preservation measures/procedures have been implicated in the outbreak, therefore measures to control the epidemic has also included campaigns to avoid certain preservation methods. Sun-drying of food is a common practice in Nigeria, especially in the Northern parts with characteristically dry and high temperature weather. Sun-drying easily exposes food to contamination by rodents, including the implicated multimammate rat. Gari is a common food delicacy in Nigeria made from cassava tubers and can be consumed by simply soaking in cold water or further prepared by cooking in hot or boiling water. It is advised that such foods be properly cooked before consumption to avoid infection.
Source: Nigeria Centre for Disease Control, (NCDC)
Other noteworthy response reported by the NCDC
Coordination: Response coordination is led by the Nigerian Centre for Disease Control (NCDC) and the Federal Ministry of Health (FMOH) with support from partners. Review meetings at the Emergency Operations Centre (EOC) and situation reports (SITREP) are conducted daily to provide updates and strategize. An Emergency National Council on Health (NCH) convened by the Honourable Minister of Health and Lassa Fever Eradication committee has been inaugurated4.
Case Management and Infection Prevention and Control: Several tablets (71,000) of Ribavirin, 20,750 vials of parenteral Ribavirin and 960 pieces of PPE have been distributed to the affected states as of January 24, 2016. Isolation centres have been identified in most states and the emergency unit at the Federal Medical Centre, Jabi was decontaminated on January 24, 2016 by the Federal Capital Territory (FCT) and NCDC team4.
Surveillance: Outbreak investigation, contact tracing and clinician training continues in the affected states. On January 23, 2016, Akwa Ibom (South Nigeria) reported a case that had been confirmed at the Institute of Lassa Fever Research Centre on January 18, 20164.
Laboratory: Five national laboratories with PCR capability are currently conducting analysis of samples with 194 samples analyzed. Of those tested, 57 have tested positive for Lassa fever while other VHFs were negative. Sixty-three (63) laboratory results are pending4.
Communication and Social Mobilization: There is a functional NCDC Call Centre while radio and television segments are ongoing. There is a website dedicated to Lassa fever information (www.lassaalert.org) linked to the NCDC website. Community health education is ongoing as part of state team responses4.
Challenges: Some challenges include coordination of laboratory network leading to delay in sending laboratory results, delayed daily reporting of cases (especially from tertiary health facilities), logistics support for contact tracing in the states, logistics for sample transportation for prompt laboratory diagnosis and low supply of Ribavirin4.
Next steps: According to NCDC, the next steps are:
- reinforcement of active surveillance, contact tracing and continued outbreak investigation
- continued clinician training and reinforcement to ensure early detection and reporting
- continued health education and community education
- resource development and policy development at state level for coordination, surveillance, case management, communication and social mobilization
- coordinating laboratory networks for prompt release of documented results4.
References:
- Centers for Disease Control and Prevention (2015, June 2). Lassa Fever. Accessed on February 5, 2016: http://www.cdc.gov/vhf/lassa/
- Granjon, L., Lavrenchenko, L., Corti, M., Coetzee, N. & Abdel-Rahman, E.H. (2008).Mastomys natalensis. The IUCN Red List of Threatened Species 2008: e.T12868A3392767. Accessed on February 5, 2016: http://dx.doi.org/10.2305/IUCN.UK.2008.RLTS.T12868A3392767.en
- Lassa Alert, 2016: Accessed on February 13, 2016 at: http://www.lassaalert.org/index.php/faq/
- Nigeria Centre for Disease Control (NCDC), 24 January, 2016: LASSA FEVER OUTBREAK IN NIGERIA; Daily Situation Report, No. 16. Accessed on February 13, 2016 at: http://www.health.gov.ng/doc/Lassa16.pdf; http://www.health.gov.ng/index.php/78-featured/106-article-e
- Nigeria Federal Ministry of Health (2016, January 8). Press Briefing on the Outbreak of Lassa fever in Nigeria by the Honourable Minister of Health. Accessed February 5, 2016: http://www.health.gov.ng/index.php/about-us/9-uncategorised
- World Health Organization (2015, March 13). Lassa fever. Fact sheet, accessed February 5, 2016: http://www.who.int/mediacentre/factsheets/fs179/en/







