



A Healthy Future for Community Pharmacy:
Lessons from Point-of-Care Testing Platforms in Canada and the United Kingdom
Introduction
In an era of escalating healthcare demands, community pharmacies have emerged as vital providers of accessible, cost-effective care. Programs like HealthTab® in Canada and Pharmacy First® in the United Kingdom (UK) exemplify the transformative potential of pharmacies in expanding chronic disease prevention and management, particularly for cardiovascular health and diabetes. Early data from HealthTab highlight its clinical benefits, yet Canada faces challenges in scaling these innovations due to inconsistent funding and policy support. By contrast, the UK’s Pharmacy First program demonstrates how robust policy frameworks and investment can amplify pharmacy-led innovations, as evidenced by HealthTab’s recent integration into NHS community pharmacy initiatives. This article explores the successes, challenges, and opportunities for advancing community pharmacy models globally, drawing lessons from Canada and the UK to inform a path toward pharmacy-led chronic disease care.
The Global Role of Community Pharmacies in Chronic Disease Management
Community pharmacists are increasingly recognized as essential frontline providers in chronic disease management worldwide. In the United States, over 90% of individuals live within five miles of a pharmacy, where pharmacists deliver critical services such as vaccinations, point-of-care testing (POCT), and chronic disease screening (American Pharmacists Association, 2023). Internationally, pharmacists are often the most accessible healthcare professionals, with evidence demonstrating their interventions improve clinical, economic, and humanistic outcomes (World Health Organization, 2023).
A meta-analysis of 39 randomized trials involving over 14,000 patients found pharmacist-led care reduced systolic blood pressure by approximately 7.6 mmHg in hypertensive patients (Santschi, 2014). In Canada, the RxEACH trial showed that pharmacist case-finding and prescribing reduced cardiovascular event risk by 21% compared to usual care (Tsuyuki, 2015). These findings, supported by organizations like the World Health Organization (WHO) and the International Pharmaceutical Federation (FIP), underscore the need for policy support and collaborative practice models to empower pharmacists in managing conditions such as diabetes, hypertension, and dyslipidemia (International Pharmaceutical Federation, 2022).
HealthTab: A Groundbreaking Initiative in Canadian Community Pharmacy
HealthTab is a POCT platform that equips Canadian pharmacists with tools for rapid, lab-quality screenings, including on-site HbA1c testing for diabetes. Integrated into pharmacy workflows, it provides real-time reporting, transforming pharmacies into convenient hubs for preventive care. A 13-week pilot across 40 pharmacies yielded significant insights:
Table 1: Key Findings from the Canadian HealthTab Diabetes Screening Pilot
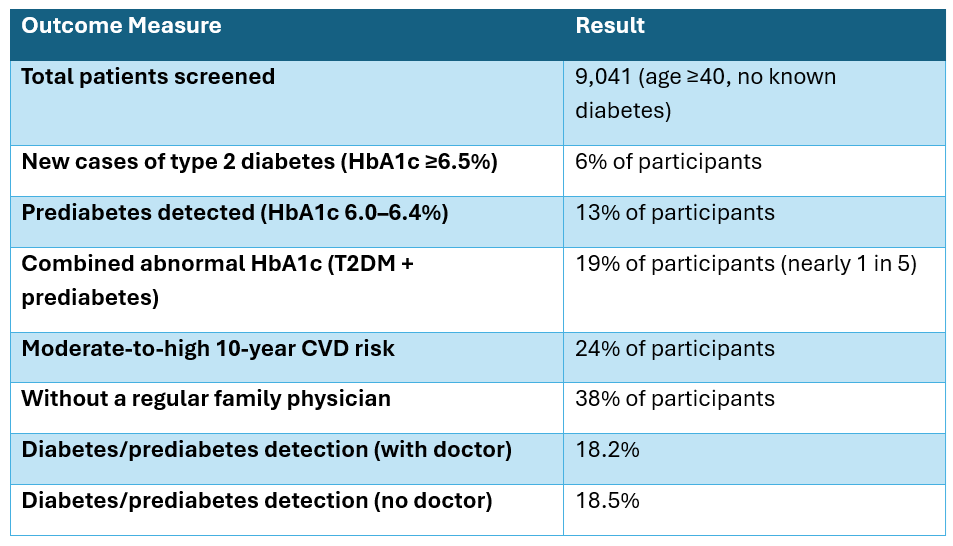
These results reveal a critical public health gap: 38% of participants lacked a regular family physician, yet detection rates for diabetes and prediabetes were nearly identical regardless of primary care access (18.2% vs. 18.5%). This suggests traditional healthcare settings miss many at-risk individuals, positioning pharmacies as vital access points for early detection (Papastergiou, 2024).
Economic and Public Health Benefits of POCT in Pharmacies
Pharmacy-led POCT offers economic viability and clinical effectiveness, particularly in early disease detection. Early intervention reduces long-term healthcare costs by identifying at-risk individuals before complications arise (NHS England, 2023). For example, NHS data estimate a £7.52 return for every £1 invested in pharmacy-led cardiovascular screening, driven by reduced emergency visits and hospitalizations (NHS England, 2023). With 90% of populations in developed nations living within five kilometers of a pharmacy, this accessibility enhances public health outcomes (International Pharmaceutical Federation, 2022). However, scalability hinges on sustainable reimbursement and integrated healthcare models.
Lessons from the UK: Pharmacy First and the Power of Policy Support
The UK’s Pharmacy First program empowers pharmacists to manage minor ailments, prescribe contraception, and screen for chronic disease risk factors, supported by government funding and standardized reimbursement (NHS England, 2024). By alleviating pressure on general practitioners (GPs), it strengthens primary care capacity while delivering cost-effective outcomes. HealthTab’s expansion into NHS initiatives further validates this model’s adaptability. The UK’s success contrasts with Canada’s fragmented landscape, where inconsistent funding and scope-of-practice variability hinder progress (Canadian Pharmacists Association, 2023).
Challenges to Scaling POCT in Canada
Despite HealthTab’s promise, scaling it across Canada faces significant barriers:
- Inconsistent Funding: Pharmacy services are tied to dispensing, with limited public funding for preventive care (Canadian Pharmacists Association, 2023).
- Scope-of-Practice Variability: Unlike the UK’s centralized framework, Canada’s provincial regulations differ, complicating national implementation (Papastergiou, 2024).
- Integration Gaps: Without shared electronic health records (EHRs), coordination with primary care remains limited (Tsuyuki, 2015).
Regulatory, Training, and Infrastructure Considerations
Successful POCT adoption requires evolved regulatory frameworks, pharmacist training, and infrastructure investment. The UK and Australia exemplify this through standardized reimbursement and training programs, enabling pharmacists to operate at their full scope (International Pharmaceutical Federation, 2022). In Canada, harmonizing scope-of-practice laws and integrating pharmacy data into EHRs are critical steps. Pharmacists need specialized training in test administration and patient counseling, supported by digital tools for seamless care coordination (Steben, 2018).
Policy Recommendations
- Sustainable Funding: Establish public funding for pharmacy-led preventive services.
- Harmonized Policies: Standardize scope of practice across jurisdictions.
- Integrated Networks: Link pharmacy services with broader healthcare systems via EHRs.
- Public Health Partnerships: Leverage pharmacies for chronic disease prevention.
Conclusion
HealthTab’s detection of diabetes risk in nearly one-fifth of screened individuals underscores the potential of community pharmacies in preventive care. However, Canada’s fragmented policies limit scalability, while the UK’s Pharmacy First program offers a blueprint for success through investment and empowerment. By adopting these lessons, Canada and other nations can redefine pharmacies as trusted hubs for chronic disease management, enhancing accessibility, improving outcomes, and reducing healthcare system strain.
References
American Pharmacists Association. (2023). The role of pharmacists in public health. Retrieved from https://www.pharmacist.com
Canadian Pharmacists Association. (2023). Scope of practice for pharmacists across Canada. Retrieved from https://www.pharmacists.ca/pharmacy-in-canada/scope-of-practice-canada/
International Pharmaceutical Federation. (2022). Expanding the role of community pharmacists in chronic disease management. FIP Report.
NHS England. (2023). Economic impact of cardiovascular screening in community pharmacies. NHS Reports.
NHS England. (2024). Pharmacy First: Expanding the role of community pharmacy in primary care. NHS England Reports.
Papastergiou, J., Elsabakhawi, M., Lori, L., Potter, C., & Van Den Bemt, B. (2024). Community pharmacy-based HbA1c screening for early detection of diabetes and prediabetes. European Journal of Hospital Pharmacy, 31(Suppl 1), A119-A120.
Santschi, V., Chiolero, A., Burnand, B., Colosimo, A. L., & Paradis, G. (2014). Impact of pharmacist care in the management of cardiovascular disease risk factors: A systematic review and meta-analysis of randomized trials. Archives of Internal Medicine, 174(11), 1859-1868.
Steben, M., Wenger, L., Raman-Wilms, L., Schneider, E., Church, D., & Waite, N. (2018). Pharmacists as immunizers, their pharmacies and immunization services: A survey of Ontario community pharmacists. Canadian Pharmacists Journal (Ottawa), 151(4), 263-273.
Tsuyuki, R. T., Houle, S. K., Charrois, T. L., Kolber, M. R., Rosenthal, M. M., Lewanczuk, R., et al. (2015). Randomized trial of the effect of pharmacist prescribing on improving blood pressure in the community: The Alberta clinical trial in optimizing hypertension (RxEACH). Circulation, 132(2), 93-100.
World Health Organization. (2023). Community-based healthcare and its role in managing chronic diseases. WHO Report.







