



Abstract:
Health care workers (HCWs) and patients are at risk of acquiring tuberculosis (TB) infection in health care facilities. Such risk characterizes TB as a dual public health threat – first as a communicable disease and secondly as an occupational health hazard. Although Tuberculosis Infection Control (TBIC) measures put in place in clinics may reduce infection transmission, implementation remains a major challenge. This case study assessed barriers to implementation of TBIC among HCWs in two South African primary care clinics in a Cape Town township with a high TB prevalence. Strengthening the health system is a key strategy in emergency preparedness and disease control. Some of the barriers were inadequate HCW training on TBIC, a non-responsive compensation policy and the perception that a busy clinic schedule leaves no time for TBIC implementation. Resource availability, adequate human resources and leadership enabled HCWs to implement TBIC. From the results, policy on paper is different from policy in practice. Health system efficiency is very much dependent on the health workforce who translate policy to practice.
Article:
This article was adapted from an original study “Barriers to Implementation of Tuberculosis Infection Control amongst South African Health Care Workers.”(Adeleke et al. 2012)
Background
Infection control is a topical contemporary Public Health issue with recent outbreaks of Lassa Fever and Zika Virus (Diamond & Ogungbire 2016, WHO, 2016). Tuberculosis (TB) is an airborne infectious disease that can be transmitted from one person to another. The burden of TB disease driven by high HIV prevalence and increased vulnerability to TB increase the likelihood and significance of health-care associated TB transmission (Wood et al., 2007, Bock et al., 2007, Shenoi et al, 2010). Health-care associated infections refer to infections that are acquired by staff or users of health services within health care facilities (Mehtar, 2010). The risk of health-care associated TB has been recognized in health care settings worldwide (Pai et al., 2006, Basu et al., 2007). Health Care Workers (HCWs) in South Africa are at risk of acquiring TB infection from their work environments (Joshi et al., 2006).
Undiagnosed and untreated TB cases are commonly found in waiting rooms of health facilities (Heysell et al., 2011; Shenoi et al., 2010; WHO 1999), thereby increasing the likelihood of health-care associated TB (Bock et al., 2007). Invariably, HCWs are an essential part of the health system; they are the key implementers of infection control policies such as TBIC.
Tuberculosis Infection Control
Infection Prevention and control- (IPC; including TBIC) is an internationally recognised and legislated prevention strategy. Provisions for IPC in South Africa are documented in Health and Safety at Work Act, Occupational Health Act, Public Health Act, Constitutional law and WHO recommendations (Mehtar, 2010). TBIC includes a combination of measures used as part of a holistic approach to effectively reduce the risk of TB transmission within crowded settings, including health care facilities (WHO 2009, Department of Health, 2004). TBIC is comprised of three categories of measures that are hierarchical, but usually implemented simultaneously to reduce the risk of health-care associated infections (WHO 2009). These measures are 1) administrative controls, 2) environmental controls and 3) the use of personal protective equipment. HCWs are seen as the front-line implementers of TBIC in health care facilities and therefore play a vital role in the effective and consistent implementation process.
Role of HCWs’ Motivation in TBIC Practice
Since HCWs are an essential part of the health system (WHO, 2007) that implements health policies within health care facilities, understanding what motivates HCWs to implement TBIC is crucial for identifying barriers to implementation. TBIC requires consistent implementation by HCWs to reduce TB transmission in clinics. Shortage of appropriately-trained HCWs and de-motivated staff are known barriers to achieving TB infection control (TBIC) targets (USAID/Stop TB 2010). A poorly motivated and inadequately trained health care workforce was a major health system barrier to achieving the Millennium Development Goal of reversing the global incidence of tuberculosis by 2015 [Padayatchi et al., 2010, WHO 2007).
In South Africa, barriers to TBIC implementation reported by HCWs include TB/HIV related stigma and resource constraints (Kanjee et al., 2012, Sissolak, Marais & Mehtar 2011). Resource availability and worker competence are not sufficient to enhance health worker performance; rather, worker motivation in service delivery is critical in ensuring sustained health worker performance (Franco, Bennett& Kanfer, 2002). Exploring barriers to TBIC implementation, this study further assessed the willingness of HCWs to maintain TBIC practices in health facilities by identifying factors that motivate and demotivate HCWs.
Methods
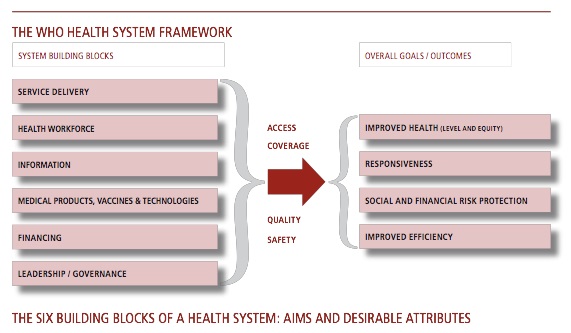
A case study design (Yin 2009, Rule& John, 2011) was used for assessing how HCWs implement TBIC in two clinics within a Cape Town Township from March to May 2012. Case study design was used to explore challenges HCWs experience while implementing TBIC within clinics so as to relate study context (clinics) to the practice being explored (TBIC). In line with the case study design, a conceptual framework (Figure 1) on HCW motivation within the work environment was further used to explore barriers to TBIC practice. Data was collected by direct observation, key informant interviews, semi-structured interviews, focus group discussions and document review. The data was analysed using thematic analysis and interpretive analysis.
Figure 1: Highlights of Study Relevance to Health System framework: The relationship between health workforce in service delivery through infection control policies (safety) leading to responsiveness and improved efficiency of the health system WHO Health System Framework (WHO, 2007).
Study Population
The study population included eight lay and eleven professional HCWs (N = 19) from two clinics. The study participants constitute 28% of all HCWs (N= 69) working in both clinics. Professional HCWs included: nurses, doctors and pharmacists working in the study clinics. Lay HCWs included clerks, nursing assistants, general workers, and educators from Non-Government Organizations (NGOs). Most professional and lay HCWs in both clinics were employed by the City of Cape Town municipality. However, one lay HCW was employed by NGOs.
Data collection and Sampling
Two clinics were selected for the study using the following inclusion criteria: a clinic with at least 15 HCWs and a patient load of at least 30 per. Based on the inclusion criteria, the staff of Médecins sans Frontières (MSF, Doctors without Borders) familiar with TBIC in the community nominated five clinics eligible for the study. Site visits were conducted to these five clinics and only three out of the five met the inclusion criteria. Two clinics (A & B) were finally selected, based on inclusion criteria and accessibility. Convenience sampling was used to recruit HCWs to compensate for the busy schedules and heavy workload in each clinic. All interviews and focus group discussions were conducted in English at the clinics by the principal researcher (first author).
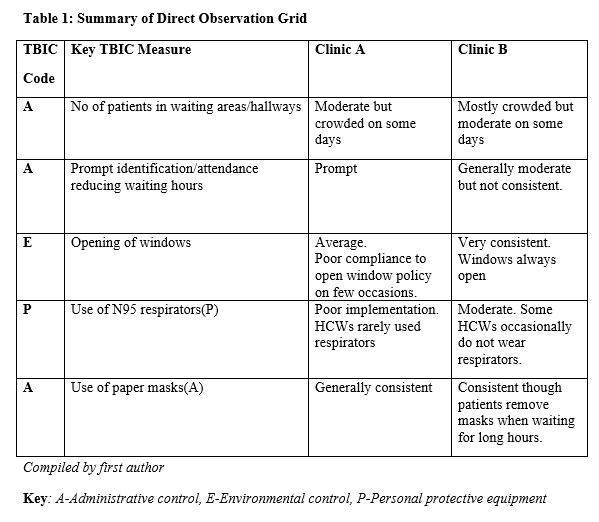
Data was collected by direct observation of HCWs implementing TBIC within clinics (5 working days per clinic), key informant interviews among facility managers and a sub-district health representative (n=3), semi-structured interviews among professional HCWs (n=7) and Focus Group Discussion (FGD) among lay health care workers (n=3). An observational grid and interview guidelines were developed as data collection instruments.
Description of Clinic A and Clinic B
Health service delivery in Clinic A was threefold: child health, women’s health and adult chronic care. Its package of care includes adult curative, child care, reproductive health, basic ante-natal care, diagnosis and treatment of sexually transmitted infections (STIs), TB as well as antiretroviral (ARV) administration. Out of a total of 39 HCWs in Clinic A, 11 health care workers participated in the study. One key informant interview, three semi-structured interviews and two focus groups were held. Only lay HCWs were initially scheduled to participate in FGDs according to the study protocol but due to work overload in the clinic, both professional and lay HCWs (working in TB section) had to participate in an additional FGD.
Clinic B provides a two-fold health service delivery: Child health and women’s health. With the exception of adult chronic care, clinic B offers services similar to clinic A. From a total of 30 HCWs in Clinic B, eight HCWs participated in the study. One key informant interview, four semi-structured interviews and one FGD were held in Clinic B. Three lay HCWs participated in the focus group discussion.
Ethics
The study, in line with the Helsinki declaration, was approved by UCT Human Research Ethics Committee and the City of Cape Town Health committee. Facility managers of both clinics were asked to participate in the study and handed a one-page research summary a week before the study commenced. All participants gave written informed consent before participating.
Data Capture
The principal researcher (first author) transcribed audio clips from interviews. A colleague (Masters in Public Health student) validated transcribed notes with audio clips so as to minimize reporting bias. Participants’ responses were clarified after interviews and during report writing (member checking) to ensure reliability of data.
Data Analyses
Data was analysed using thematic analysis and interpretive analysis (Yin 2009, Rule & John, 2011). Prior TBIC assessment reports (MSF 2011) of both clinics were compared with data from case study research during analysis. A codebook was manually developed with themes generated from the interview guidelines and the themes which emerged from HCWs’ responses. Filter questions were incorporated into interview guidelines to ensure data reliability. For example, “what enables you to implement TBIC?” is a filter question to “what motivates you to implement TBIC?”
Based on a motivation framework developed from the literature on TBIC implementation (Figure 1), factors that motivate HCWs to implement TBIC were identified from precede-proceed model and work motivation theory (Franco, Bennett& Kanfer 2002, Green & Keuter 1999). Although we sought to explore barriers to TBIC practice, we also identified potential enablers from HCW responses and direct observation.
Results and Discussion:
Demographic Characteristics of participants
More female (n=14) than male (n=5) HCWs participated in the study. The number of professional female HCWs (n=7) and lay female HCWs (n=7) who participated in the study was the same. Only one male lay HCW participated in the study, the other four were professional HCWs. Of all participants, 11 were professional HCWs while 8 were lay HCWs. Respondents’ levels of education varied from Grade 10 to a Masters degree, with most having professional medical/nursing degrees. The highest level of education for lay HCWs was secondary schooling (Grade 12) while professional HCWs had post-secondary education. The number of years worked in health care facilities ranged from two weeks to thirteen years, with an average of one year across respondents. Lay HCWs had worked in the clinics longer than most professional HCWs. Of the nineteen HCWs interviewed in both clinics, nine worked solely in the TB section of the clinic. The age of respondents varied between 27 and 60 years. Lay HCWs were much older (34-60 years) than professional HCWs (27-55 years) in both clinics.
The results are discussed and grouped under two main headings: Policy and Practice. The national and facility specific policies that guide TBIC practice are discussed first. Next are the enablers and barriers to TBIC practice in Clinic A & Clinic B.
Policy
There are two key policies for TBIC implementation in the study clinics: a TBIC facility specific policy (designed under an MSF project) and an open window policy (supports environmental control). Findings related to ‘open window policy’ will be discussed under environmental control measures. Facility specific TBIC policies were publicly displayed on the walls of the waiting room and the facility manager’s office in both clinics in the form of a poster. Some professional HCWs indicated they were aware of facility specific TBIC policy guiding implementation but stated that it only emphasized personal protective equipment for TBIC.
There is a TBIC policy that emphasizes wearing of respirators by HCWs. If our superior officer visits, we run to get our masks, we know what the policy states.
– P15-Professional HCW
As at March 2012, South Africa was one of several countries that are yet to finalize a National TBIC plan (WHO 2011). A draft national policy has been developed since 2007 (Department of Health). HCWs employed by NGOs independent of the City of Cape Town seem to have internalized infection control policy as a reinforcing factor (Figure 1) that helps them maintain TBIC practices as voiced by this respondent:
No one is supervising. But because I was employed by an NGO, in our contract, they wrote that if they catch you not wearing ‘masks’, you will be sanctioned, so it is my responsibility.
– P16-Lay HCW
There is still a gap in policy implementation among HCWs. Policy as an intent is different from policy in practice. Although facility specific TBIC policies have been developed, HCWs still need to understand the hierarchy of implementation and take responsibility for consistent implementation similar to the NGO employee. Sub-district health systems can learn from NGOs’ training strategies that contribute to sustained policy implementation among HCWs. The national TBIC plan needs to be finalized as a standard of TBIC practice. A national policy on TBIC would underline infection control as a national priority. If well implemented, such a policy can prevent TB transmission in clinics and other settings.
Enablers of TBIC implementation among HCWs
Resource availability
Professional and lay HCWs are more likely to implement TBIC when resources are provided in the form of infrastructure, human resource and consumables (e.g., N95 and paper mask). Professional HCWs mentioned the crucial role of human resource availability in TBIC practice, especially with regards to reduced workload per staff member, leaving more time to implement TBIC.
Last year, we asked for more staff, we are happy because they have recruited more people, now we can listen to TBIC, we have more people and more time to implement.
– P3-Professional HCW
Key informant interviews revealed that proper supply of stock was linked to transport and logistics support relating to the regular supply of consumables. Implementation of TBIC among HCWs was also determined by enabling factors. Health system support characterized by leadership, resource availability, operational policies enabled HCWs to implement TBIC. This finding is in line with previous research that organizational support and commitment to health workers’ safety strongly motivates HCWs to implement TBIC (Kanjee et al., 2012, Yassi et al., 2007).
Leadership by delegation-Infection Control Committee
As a further administrative control measure, a facility manager assigned responsibility for IC to a professional HCW as the ‘head of the infection control committee’. Such delegation, combined with on-going supervision, seemed to have emphasized TBIC as a priority in Clinic B compared to Clinic A where infection control committee was yet to be functional.
There is someone I have given the portfolio to who is championing IC. He is the one doing IC audit on a monthly basis and then we discuss it with the general assistants.
– P4-Professional HCW
Supervision
It was observed that HCWs in clinic B used respirators more consistently compared to clinic A. Key informant interview revealed that in Clinic B, the facility manager who had earlier observed the inconsistent use of respirators among HCWs organized a fit-test of ‘N95 respirators’ to encourage sustained use of respirators among staff. The fit test enabled HCWs to use respirators as indicated by this respondent:
Last year, we had fit testing sessions. I asked the TB/HIV coordinator to come and do a fit test for all the staff- those working in the TB room. So it fits them properly.
– P5-Professional HCW
Although HCWs’ discomfort while using respirators can be subjective according to individual needs and preferences which the health system may not be able to address, fit tests can minimize discomfort by helping HCWs to identify most suitable respirators.
After the fit-tests, one of the HCWs working in the TB unit was seen not wearing a respirator. The manager then requested a signed document stating the HCW was not willing to use the PPE provided by the district health system. This punitive approach seems to work because the same HCW began wearing a respirator during later observations. HCWs need to be supervised and constantly reminded about maintaining TBIC practices in clinics. However, HCWs tend to be influenced by the social norm when colleagues wear PPE. One HCW declared:
…[in] this particular clinic, I see that everybody wears a mask more than in other clinics which is encouraging….I think when you are working with people who are conscious of IC, it makes you more conscious of IC.
– P6-Professional HCW
Similar to our findings, a recent South African study associated staff motivation such as support from colleagues with implementation of TBIC among HCWs (Kanjee et al., 2012). In-service training could be a potential platform to garner support for implementing TBIC in clinics.
Fear
Fear of getting TB was the most commonly reported factor that motivates both lay and professional HCWs to implement TBIC measures.
Yes, MDR-TB, that’s why you have seen me trying to wear masks these days… I think that is like really scaring us now, because you know what, I don’t know when a client comes in if he has MDR or not.
– P1-Professional HCW
Based on the motivational theory (Figure 2), fear is a predisposing factor to implementing TBIC among both lay and professional HCWs in both clinics.
HCW screening for TB
On HCW screening for TB, the health system makes diagnostic services readily available to staff. TB screening is voluntary and usually initiated by HCWs. When asked if TB screening is available to HCWs, one of the interviewees responded:
We are allowed to whenever you feel like. If I feel like I want to cough or have an x-ray because maybe I am suspecting, that [resource] is in place.
– P3-Professional HCW
Such provision of TB screening services to HCWs is an enabling factor (Figure 2) for TBIC practice. If HCWs are provided with needed services that enhance their health such as screening for TB, they are more likely to feel supported by the health system and implement TBIC. If screening services were unavailable, HCWs are likely to feel de-motivated.
Barriers to TBIC implementation among HCWs
Non-responsive Compensation policy
Another de-motivating factor expressed by HCWs was the non-responsive compensation policy, should they ever get active TB disease. Compensation for active TB disease is a regulatory factor (Figure 2) that can motivate HCWs to sustain TBIC practices by being financially responsible for their TB disease. Although TB is a compensable disease according to the Compensation for Occupational Injuries and Diseases Act (COIDA), one HCW commented:
The thing is with TB and being a health worker, should I get it, I know it’s gonna be my problem. I won’t be able to prove that I got it here. There is nothing in place that says if you are working in TB dept, you will be compensated. So I guess if you work here, it is at your own risk, that’s how I feel.
– P3 -Professional HCW
A finding from a key informant interview revealed that HCWs are not required to prove the infection was health-care associated. Further probing on the nature of compensation HCWs expect from the health system revealed both financial and non-financial.
It could come in many different ways, remuneration is always a good thing, give me more money, sometimes recognition, even if it’s not in form of money.
– P3-Professional HCW
Compensation for Occupational Injuries and Diseases Act (COIDA) policy serves as a regulatory document that supports reimbursement of HCWs who develop TB disease. Because of bureaucratic process and delays, HCWs see TB as a ‘personal problem’ and not an institutional problem. Previous research suggests that such lack of trust in the system can be a barrier to motivation (Gilson 2003) of HCWs who implement TBIC.
No time for TBIC
Both professional and lay HCWs perceive TBIC as a separate agenda from their routine tasks that they are being mobilized to support. Some professional HCWs relate TBIC implementation to HCW being paranoid particularly in such a busy environment which is already challenging. Although HCWs perceive they are at risk of getting TB and particularly dread being infected with Drug Resistant-TB, they feel too busy to adhere fully to TBIC measures. It appears as though professional and lay HCWs are initially motivated by fear to implement TBIC but become so familiar with the working environment that the perceived risk of acquiring TB wanes over time. This perception suggests that TBIC is yet to be prioritized and integrated into service delivery procedures in clinics as illustrated by this respondent:
I used to be scared when I started but I have gone past that now…like yesterday we were so busy here, no time to get paranoid.
– P12-Professional HCW
HCW perception of TB concentration in certain clinic sections
Lay HCWs not working in the area of TB did not see a need to use PPE because they did not perceive they are at high risk of acquiring TB. In Clinic A, lay HCWs (assisting the TB team) did not use respirators while attending to patients because of their perceived low risk of contracting TB. Further probing on the possible reasons for the perceived low risk revealed that HCWs associate consistent use of respirators with HCWs working in TB sections or working with diagnosed TB patients. As far as they are concerned, TB is concentrated in one section of the clinic: the TB ward.
Therefore, the perception is that spending a few minutes in the TB room does not predispose them to TB infection as stated by these respondents:
I don’t work in TB room full time, just helping out so I don’t need to wear masks.
– P9-Lay HCW
This perception that an airborne infection such as TB is only restricted to the TB section of the clinic is a barrier to TBIC implementation among HCWs that needs to be addressed during staff meeting and by displaying IEC posters in all sections of the clinic. For example a poster that reads ‘TB somewhere in the clinic is TB everywhere in the clinic: are you protecting yourself?’ can be posted in each section of the clinic to inform HCWs and clients.
Training deficit
According to facility specific policies on TBIC, in-service training is an administrative control measure. Most professional HCWs had not received further training on TBIC. However, two professional HCWs had attended one-day training on TBIC organized by NGOs. Although prior needs assessment report in both clinics have identified refresher training as integral to improved infection control, in-service training is yet to be implemented in these clinics. Two predisposing factors (Figure 1) that determine sustained TBIC practice are HCWs’ perception of risk and the training they have received on TBIC. If HCWs perceive they are at risk, they are more likely to participate in training and implement TBIC in a consistent manner. Research suggests that improvements recorded in the ‘work and systematic training’ of health workers at primary health care level contributed to successful TB control (Abreu et al. 2011). Studies have also shown the benefit of in-service training result in improved TB care in resource constrained settings within South Africa (Fairall et al. 2005). Sustained TBIC implementation requires training focused on behavior change communication, rather than knowledge acquisition (Green & Keuter 1999). In-service training can easily bridge the gap between knowledge and practice identified as a barrier to TBIC practice in previous studies (Kanje et al. 2012, Fairall et al. 2005, Farley et al. 2012). In line with Berhe’s findings in 2005, in-service training could be more effective if designed to meet various needs of lay and professional HCWs.
Lack of shared responsibility among HCWs
Although all interviewed HCWs in one of the clinics knew there was an IC committee, they seemed to be detached and unaware of the actual committee activities. The head of the IC committee works in another section of the clinic, rather than in the TB section itself. When interviewed, the head of the IC committee stated a barrier to TBIC as over-reliance and lack of shared responsibility among other HCWs by stating:
The barrier is that they tend to rely on one person….it should be done by everybody. It should start with me and extend to everybody. It should be everybody’s responsibility.
– P14-Professional HCW
There is need to re-sensitize HCWs about their contributing role to effective TBIC practices in clinics. The leadership of IC committees could be rotated across various departments to encourage HCWs to develop a sense of responsibility towards infection control.
Non-proactive use of PPE- respirators
An important finding is the non-proactive way HCWs use respirators by only wearing them after they know the TB status of a patient.
I only wear mask when I know a patient has been diagnosed. It is suffocating, a communication barrier and feels hot.
– P8-Professional HCW
Such non-proactive use of respirators reflects a lack of understanding as to who is more likely to be infectious. Undiagnosed and untreated TB cases that will be infectious are mostly found in the waiting areas of clinics (Shenoi, Escombe, Friedland, 2010). Wearing respirators only for known TB cases is therefore a barrier to consistent TBIC implementation among HCWs.
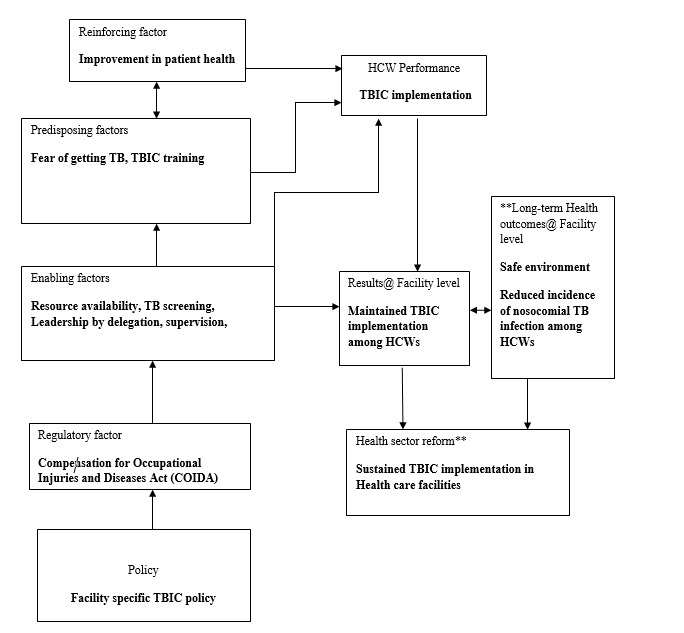
Figure 2: Motivation framework of TBIC implementation among HCWs
Adapted from Work Motivation in the organizational context (Franco et al., 2002) and Precede-Proceed model (Green and Kreuter, 1999)
**Long term indicators not considered in the study
Limitations:
This study had several limitations. Purposive sampling of cases (clinics) may have introduced a form of selection bias. Bias was minimized by selecting multiple clinics and reporting enablers alongside barriers to TBIC practice. Key findings are based on HCWs’ self-reported barriers to TBIC implementation and direct observation. However, collected data was compared with prior TBIC clinic assessment reports. Interpretation of qualitative data is often regarded as subjective. To minimize reporting bias, participants’ responses were verified during report writing.
Another limitation was that interviews and FGDs were in English. Even though all HCWs could speak English, speaking a local language may have generated more data due to cultural affinity. However, a HCW assisted the researcher to interpret Xhosa phrases spoken by some lay HCWs during FGDs.
In addition, the conceptual framework on HCW motivation (Figure 1) did not consider long term indicators** such as reduced incidence of health-care associated TB infection among HCWs and sustained TBIC implementation in health care facilities. This will require longer study period to observe daily implementation beyond a few working days. This study is applicable to other primary care clinics within the community studied. This is because other primary care clinics have similar staff profile and comparable working conditions. Study findings can be relevant to Cape Town, South Africa at large because of they are governed by the same national health system. However no two clinics are exactly the same. Each clinic may differ in leadership style, HCW motivation and other contextual differences.
Finally, it is difficult to transfer case study research to other settings internationally (e.g other African countries) without considering the uniqueness of such setting such as health system.
Summary:
Identified barriers and enablers to TBIC implementation were linked with health systems and HCW motivation. Some of the barriers were inadequate HCW training on TBIC, a non-responsive compensation policy and the perception that a busy clinic schedule leaves no time for TBIC implementation. Resource availability, adequate human resources and leadership enabled HCWs to implement TBIC. Measures such as use of respirators and masks tend to be prioritized by HCWs ahead of administrative and environmental measures that are potentially more effective in reducing TB infection.
Conclusion and Significance:
HCW motivation plays a crucial role in consistent implementation of TBIC measures. In-service training and leadership characterized by delegation with supervision could motivate HCWs. Further research should focus on identifying behavioural models that further explain barriers to TBIC implementation among HCWs and how to address these barriers despite patient workload, insufficient HCWs and other resource constraints that characterise poor urban townships.
Acknowledgement
Health Care Workers for their participation amidst busy schedule; Hanna-Andrea Rother and Helen Cox for their excellent supervision and commitment to the research.
References:
- Abreu G, González J, González E, Bouza I, Velázquez A,et al. (2011) Cuba’s Strategy for Childhood Tuberculosis Control, 1995-2005. MEDICC review 13:29-34.
- Basu S, Andrews J, Poolman E, Gandhi N, Shah Net al. (2007) Prevention of nosocomial transmission of extensively drug-resistant tuberculosis in rural South African district hospitals: an epidemiological modelling study. The Lancet 370::1500-1507.
- Berhe M, Edmond M, Bearman G (2005) Practices and an assessment of health care workers’ perceptions of compliance with infection control knowledge of nosocomial infections. American Journal of Infection Control 33:55-57
- Bock NN, Jensen PA, Miller B, Nardell E. (2007) Tuberculosis Infection Control in Resource-Limited Settings in the Era of Expanding HIV Care and Treatment. Journal of Infectious Diseases 196:S108-S113.
- Diamond L, Ogungbire A. (2016). Lassa Fever Outbreak Hits Nigeria. Infection control tips https://infectioncontrol.tips/2016/02/14/lassa-fever-outbreak-hits-nigeria/
- Department of Health. Need country and city (2004) The South African National Tuberculosis Control Program Practical Guidelines. Available: http://www.kznhealth.gov.za/chrp/documents/Guidelines/Guidelines%20National/Tuberculosis/SA%20TB%20Guidelines%202004.pdf Accessed 25 July 2012
- Fairall L, Zwarenstein M, Bateman E, Bachmann M, Lambard C, Majara B et al. (2005) Effect of Educational outreach to nurses on Tuberculosis case detection and primary care of respiratory illness: pragmatic cluster randomised controlled trial. British Medical Journal 331: 750-754
- Farley J, Tudor C, Mphahlele M, Franz K, Perrin N. et al. (2012) A national infection control evaluation of drug-resistant tuberculosis hospitals in South Africa. The International Journal of Tuberculosis and Lung Disease 16: 82-89
- Franco L, Bennett S, Kanfer R. (2002) Health sector reform and public sector health worker motivation: a conceptual framework. Soc Sci Med 54:1255-1266.
- Gilson, L (2003) Trust and the development of health care as a social institution. Social science and Medicine 56:1453-1468
- Green, L. W., and Kreuter, M. W. (1999) Health Promotion Planning: An Educational and Ecological Approach, 3rd edition. Mountain View, CA: Mayfield
- Heysell S, Moll A, Gandhi N, Eksteen F, Babaria P, et al. (2010) Extensively drug-resistant Mycobacterium tuberculosis from aspirates, rural South Africa. Emerg Infect Dis. 15:557-560.
- Joshi R, Reingold A, Menzies D, Pai M (2006) Tuberculosis among health-care workers in low and middle-income countries: A systematic review. PLoS Med 3:2378-2391.
- Kanjee Z, Amico K, Li F, Mbolekwa K, Moll A et al. (2012) Tuberculosis infection control in a high drug-resistance setting in rural South Africa: Information, motivation, and behavioural skills. Journal of Infection and Public Health 5: 67-81
- Mc Carthy K, Mosendane T, Tellie M. (2009) Implementing TB infection control in Health Care Facilities. RHRU Johannesburg.
- Mehtar S (2010) Understanding Infection Control. Cape Town: Juta Publishers.chap.1: 2,9;chap,4:158-160,172-173: chap 7:320-325
- Medecins Sans Frontieres, City of Cape Town Health (2011). Scaling up diagnosis and treatment of drug-resistant tuberculosis in Khayelitsha, South Africa: an integrated community-based approach
- Ogungbire A, Diamond L (2016). Lassa Fever Outbreak Hits Nigeria. Infection Control.tips https://infectioncontrol.tips/2016/02/14/lassa-fever-outbreak-hits-nigeria/
- Padayatchi,N, Naido K, Dawood H, Kharsany ABM, Abdool Karim Q. (2010) A Review of Progress on HIV, AIDS and Tuberculosis .South Africa Health Review 87:100. Available: http://www.hst.org.za/sites/default/files/Chap9.pdf Accessed May 5, 2011.
- Pai M, Kalantri S, Aggarwal A, Menzies D, Blumberg H (2006) Nosocomial tuberculosis in India. Emerg Infect Dis. 12:1311–1318.
- Rule, P John, V. (2011) Your guide to case study research. Pretoria: Van Schaik Publishers
- Shenoi SV, Escombe AR, Friedland G. (2010) Transmission of Drug-Susceptible and Drug-Resistant Tuberculosis and the Critical Importance of Airborne Infection Control in the Era of HIV Infection and Highly Active Antiretroviral Therapy Rollouts. Clinical Infectious Diseases 50:S231-S237.
- Sissolak D, Marais F, Mehtar S. (2011) TB infection prevention and control experiences of South African nurses – a phenomenological study. BMC Public Health 11:262.
- USAID/STOP TB. 2010, “An Advocacy Strategy for Adoption and Dissemination of the WHO Policy on TB Infection Control in Health-Care Facilities, Congregate Settings and Households.” Available from: http://www.stoptb.org/wg/tb_hiv/assets/documents/TB%2520IC%2520Advocacy%2520Strategy%2520Final%2520April%25202010.pdf [Accessed April 30, 2010]
- Wood R, Middelkoop K, Myer L, Grant AD, Whitelaw A et al. (2007) Undiagnosed Tuberculosis in a Community with High HIV Prevalence: Implications for Tuberculosis Control. Am J Respir Crit Care Med 175:87-93
- World Health Organization (2007) Everybody’s business; strengthening health systems to improve health outcomes. WHO framework for action. Geneva:WHO
- World Health Organization (2009) WHO Policy on TB Infection Control in Health care Facilities, congregate settings and households., Geneva:WHO
- World Health Organisation (2016) Question & Answer: Zika Virus. World Health Organization. http://www.who.int/features/qa/zika/en/
- Yassi A, Lockhart K, Copes R, Kerr M, Corbière M. et al (2007) Determinants of Healthcare Workers’ Compliance with Infection Control Procedures, Healthcare Quarterly 10:44-52
- Yin, R.K. (2009) Introduction. In: Case Study Research: Design and Methods. Thousand Oaks, USA: Sage
- Adeleke O, Rother H, Cox H. (2012) Barriers to implementation of Tuberculosis Infection Control among South African Health Care Workers. Chapter 16, South Africa Health Review Journal 2012/13 http://www.hst.org.za/sites/default/files/CHAPTER16_BarriersTb.pdf







