



Peer Reviewed
Cite as: Christine Greene, MPH PhD, Bryan D. Schindler, PhD. (2020) Efficacy of Ultraviolet Light Coupled with Ozone as a Germicidal Against Eight Healthcare Associated Environmental Pathogens. InfectionControl.tips.
Abstract
Background
Floors are a significant source of contamination. In hospitals, shoes act as a vector for moving pathogens into critical areas and shoe soles are never disinfected.
Aim
The aim of this study was to evaluate the efficacy of a shoe sanitizing device that uses ultraviolet light (UV-C) plus ozone for the reduction of eight clinically relevant microorganisms from a shoe sole surrogate at three exposure times.
Methods
Hard, dark rubber rubber carriers were used as a shoe sole surrogate and inoculated with approximately 1×105-7 colony forming units (CFU) of inoculum per surface carrier. Eight microorganisms were tested individually: E. coli, P. aeruginosa, MRSA, VRE, CRE, C. auris, A. brasiliensis and C. difficile spores. Test carriers were exposed to 6, 8 and 10 seconds of UV-C plus ozone using a portable foot-ware sanitizer. The total number of CFU were obtained and analyzed to evaluate log reductions and determine the optimal exposure time.
Results
A 1.42 log10 reduction was achieved for A. brasiliensis after 10 seconds of exposure. A > 3 log10 reduction was achieved for all remaining microorganisms after 8 seconds. A > 4 log10 reduction was achieved after 10 seconds for all remaining microorganisms except for VRE where a 3.86 log reduction was attained.
Conclusion
UV-C disinfection coupled with ozone provided statistically significant reductions in all microbial species tested except for A. brasiliensis.
Abbreviations
CFU – colony forming unit
UV-C – Ultraviolet Light type C
Introduction
The transmission of healthcare associated pathogens can occur through multiple environmental routes, primarily hands, surfaces, air and water. According to the CDC, approximately 1 out of every 31 patients in the United States acquires at least one healthcare-associated infection (https://www.cdc.gov/hai/data/index.html). Although environment surfaces are a known source of contamination, floors and shoe soles traditionally have not been considered a significant contributor to environmental transmission of microorganisms. Recent studies show that floors and shoes are contaminated with hospital-associated pathogens and contribute to the movement of pathogens within the hospital facility. For example, a 2014 study performed at the Clinical Department of General and Oncological Surgery UM in Poland identified Methicillin-resistant Staphylococcus aureus (MRSA) and Enterococcus faecalis on the shoe soles of 56% of physicians before rounds and 65% after rounds using swab cultures (1). A 2016 study evaluating floor contamination recovered Vancomycin resistant Enterococcus (VRE) from 69% of the hospital floor samples with no evidence of a clinical outbreak at the time of sampling (2). A review article by Rashid et al (2017) reports that almost all the 30 studies evaluated had identified hospital associated microorganisms on the floors, including MRSA, Clostridioides difficile, and multidrug-resistant Gram-negative species (3). In a separate meta-analysis, they note that transmission modes were not limited to direct contact suggesting that contamination on floors and surfaces can become airborne, particularly with increased human movement such as walking (4). Despite the growing evidence of the role of floors in environmental transmission in hospitals, there is little guidance on proper floor maintenance and cleaning for infection prevention. In fact, an EPA-registered hospital disinfectant or detergent designed for general cleaning purposes is only recommended for floors when cleaning body fluids from the floor if there is potential for presence of multi-drug resistant organisms (5).
Ultraviolet light (UV-C) technologies exist that specifically target the shoe soles for disinfection. Such technologies can help reduce the risk of transmission, particularly in critical care areas such as in operation theaters and surgical units. UV-C irradiation has been shown to be an effective germicide, is useful for targeting areas that are not routinely cleaned and is frequently used in healthcare as an adjunct disinfection method to complement the existing cleaning and disinfection protocols. Various applications of UV irradiation are employed to help disinfect air, water, and surfaces, including medical devices and instruments. The most effective germicidal wavelength range is 240-280 nm, but lower wavelengths such as 205 nm have been shown to be effective with reduced human risk of radiation exposure (6, 7). The mechanism of action involves the destruction DNA by breaking molecular bonds but efficacy is not a function of wavelength alone. Other important factors include exposure time, distance between the UV-C source and the targeted surface and directness of line-of-site (6, 8). In addition, the type of microorganism being targeted is also an important consideration. UV-C is more effective against vegetative bacteria than endospores which are structurally and chemically more complex. Spores and other fungal microorganisms have a tough outer cell wall that is difficult for UV-C to penetrate. Studies have shown that 5 minutes of direct UV-C exposure is effective at providing a >4 log reduction of MRSA on surfaces compared to 10 minutes of direct exposure to achieve a 2-3 log reduction for C.difficile spores (8).
UV-C radiation under 200 nm wavelength can create ozone from oxygen by disassociating the O2 molecule into two oxygen atoms. The single oxygen atoms will combine with available O2 molecules creating ozone (O3). Specific types of glass are typically used in the manufacture of UV-C devices that inhibit the production of ozone during use for safety purposes. Ozone is an unstable gas that has been shown to be very effective for the disinfection of a range of microorganisms including bacterial spores, fungal spores, protozoa as well as vegetative bacteria. The mechanism of action of ozone is via the oxidation of the fatty acids in the cell membrane and macromolecules (9). The application of ozone as a germicidal agent has been seen for the treatment of water, air, surfaces and even wounds. Like UV-C radiation, the effectiveness of ozone as a germicidal is dependent on dose, exposure time and distance between the ozone source and targeted surface. Given what is known about the germicidal capabilities of UV-C irradiation and ozone, the combination of the two to disinfect surfaces is a promising concept. The purpose of this study was to test the efficacy of a device that utilizes ozone with UV-C irradiation technology to disinfect the soles of shoes.
Materials and Methods
The efficacy of a portable foot sanitizer (PathO3Gen Footwear Sanitizing Station FSS-1, Future Development and Design Corp, Tampa, FL) that produces ozone (independent test data, Ozone Solutions Inc., 2019) and emits ultraviolet light (UV-C) in the wavelength range of 185 to 254 nm was evaluated against eight microorganisms: Escherichia coli ATCC 11229, Pseudomonas aeruginosa ATCC BAA-2108, Methicillin-resistant Staphylococcus aureus (MRSA) ATCC 33592, Vancomycin-resistant Enterococcus faecalis (VRE) ATCC 51299, Carbapenem-resistant Klebsiella pneumoniae (CRE) ATCC BAA-1705, Candida auris CDC B11903, Aspergillus brasiliensis ATCC 16404 and Clostridioides difficile ATCC 43598.
Culture Preparation: For S. aureus, E. faecalis, K. pneumoniae, and E. coli, all strains were propagated onto Tryptic Soy Agar with 5% Sheep Blood (SBA) and were incubated at 35 ± 2°C for 24 ± 2 hours. C. auris was propagated onto SBA at 25 ± 1°C for 18-24 hours and daily transfers were performed using Sabouraud Dextrose Agar with Letheen (SDA/L). Aspergillus brasiliensis was propogated on SDA/L for 5 to 7 days. After incubation, the A. brasiliensis culture was washed with 0.85% saline with tween and filtered with through sterile gauze. The culture was centrifuged at 4,500 rpm and the resulting pellet was rehydrated with Phosphate Buffered Saline (PBS). The Clostridioides difficile spore suspension was prepared using the U.S. EPA OPP: MB-28 (December 2017) Procedure for the Production and Storage of Spores of Clostridioides difficile for Use in the Efficacy Evaluation of Antimicrobial Agents based on ASTM Standard E2839-11.
In triplicate, sterile test carriers were inoculated by spreading 0.1 mL of a standardized suspension (1×106-8 CFU per mL) of the challenge microorganism across the entire carrier surface within a 0.25-inch margin. The carriers were allowed to dry for 60 ± 5 minutes. Control carriers for each microorganism were prepared and processed in triplicate exactly as test carriers but were not exposed to the UV-C device. After drying, the test carrier was aseptically placed inoculum side down onto the floor disinfection device using sterilized forceps. The disinfection device was sterilized using isopropyl alcohol prior to each test and sterile, hard, dark rubber carriers (2” x 2” in size) were used to simulate shoe soles.
To simulate an average body weight, a single volunteer weighing approximately 150 pounds was used for each test. For each test, the volunteer stood onto the test carrier (with a sterile barrier between the individual and test carrier) for the exposure time. Exposure times of 6, 8 and 10 seconds were tested for each microorganism. The instrument automatically shut off after the exposure time. After each exposure time, each test carrier was placed into PBS using sterile forceps, vortexed to elute the microorganisms from the carrier followed by serial dilution using PBS. Three carriers were tested per each microorganism. For each microorganism-exposure time combination, one control carrier was processed at the same time as test carriers. For bacteria, dilutions were plated via pour plate method in duplicate on Microbial Content Test Agar and incubated for 48 ± 3 hours at 35 ± 2°C. For fungi, dilutions were plated via pour plate method in duplicate on Sabouraud Dextrose Agar with Letheen and incubated for 5 to 7 days at 25 ± 2°C. For spores, dilutions were plated in duplicate via spread plate method on Brucella Blood Agar and incubated using an anaerobic chamber for 48 ± 3 hours at 36 ± 2°C. After incubation, colonies were counted, and data recorded. The mean CFU/carrier was calculated from the duplicated agar plates and the geometric mean was used to calculate the mean CFU/carrier for each organism/exposure combination. Log and percent reduction were calculated using the positive control counts. Statistical analysis was performed using GraphPad Prism, version 8.2.1 (2019).
Results
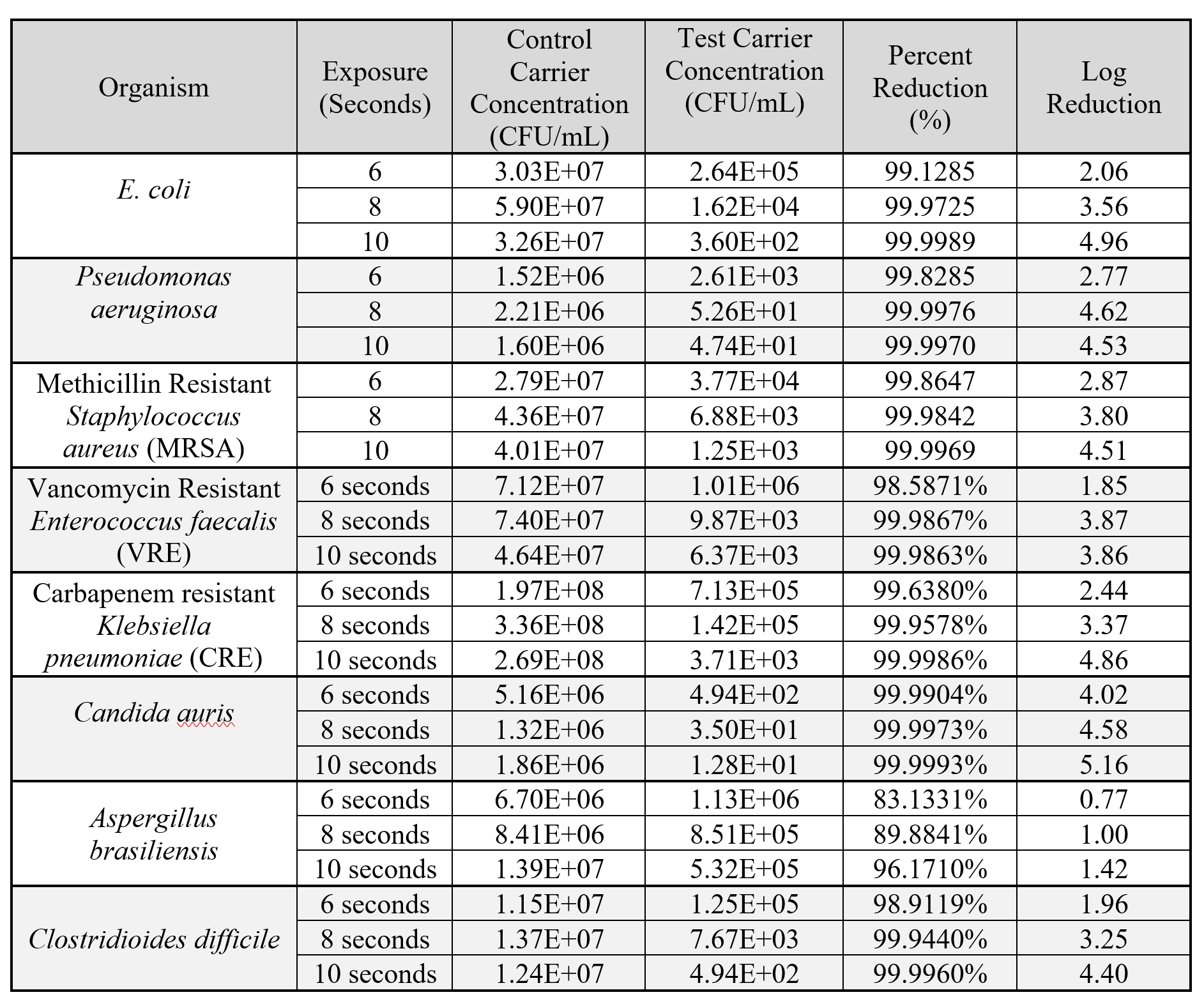
Table 1. Geometric mean of the concentrations of viable test microorganism from unexposed control carriers (n=1, plated in duplicate) and exposed test carriers (n=3, each plated in duplicate) after 6, 8 and 10 seconds.
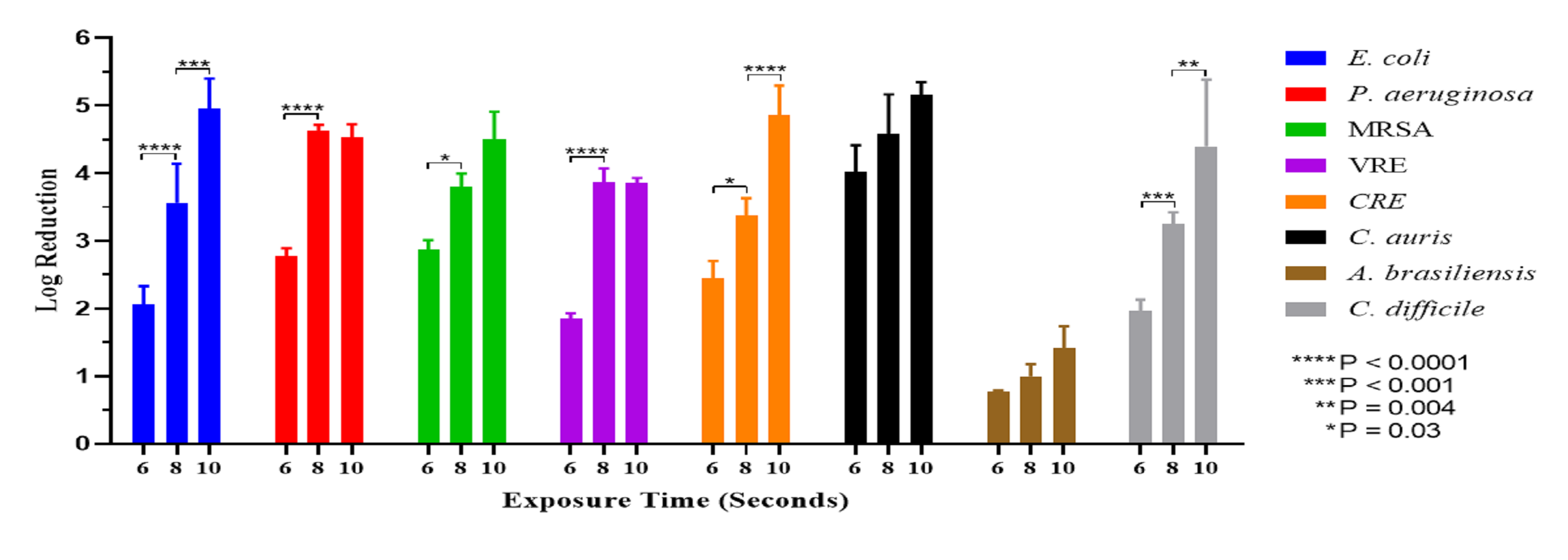
Figure 1: Mean log reduction (n=3) for eight (8) microorganisms after 6, 8 and 10 seconds of exposure.
Discussion
UV-C irradiation has been shown to be an effective germicidal that is a useful adjunct to the disinfection protocols of surfaces in the food and healthcare industries. The device used in this study uses a combination of special glass and a range of wavelengths to produce ozone with UV-C irradiation directed at the shoe sole. This study evaluated the efficacy of the combined effect of the ozone with the UV-C irradiation. Overall, we achieved mean log10 reductions of 3.87, 3.80 and 3.25, respectively (Table 1).
Three spore forming microorganisms were tested in this study; Clostridiodes difficile a spore forming, gram-positive, obligate anaerobe bacteria, Candida auris, a type of yeast that can cause severe and invasive infections and Aspergillus brasiliensis (formerly known as Aspergillus niger), a fungi that contains melanin in their conidial cell wall making it capable of absorbing UV light (11). Of these, the combination of UV-C irradiation plus ozone was most effective against C. auris, achieving a 4.02 log10 reduction after only 6 seconds. For C. difficile, at least 8 seconds of exposure were needed to observe a > 3 log10 reduction. For Aspergillus, after 10 seconds of exposure, only a 1.42 log10 reduction was achieved (Table 1). A 2011 study demonstrating the effectiveness of ozone against Aspergillus brasiliensis showed that significant reductions in A. brasiliensis did not occur below an ozone concentration of 3 g/m3 with 1 min of exposure (9). A separate study evaluating the effect of 254 nm UV-C on Aspergillus found that a 12-fold exposure time (180 seconds) was needed to achieve a >3 Log10 reduction compared to other spore forming species which required only 15 seconds (12). Therefore, even when used in combination, an exposure time of much longer than 10 seconds would be needed to observe greater reductions in Aspergillus ssp.
UV-C shoe disinfection devices on the market today have a pre-determined exposure time programmed into the device which is typically 8 seconds. Comparative studies providing data to support 8 seconds as the optimal exposure time at a given wavelength could not be found. Therefore, we tested three different exposure times (6, 8 and 10 seconds) for 8 different clinically relevant microorganisms to determine the optimal exposure time for this device. We found a statistically significant increase in log10 kill at 8 compared to 6 seconds for six of the eight microorganisms tested (Figure 1) and the differences in log10 kill at 10 compared to 8 seconds were statistically significantly increased for three microorganisms. A greater than 4 log10 reduction was achieved after 10 seconds for 6 of the microorganisms tested (E. coli, P. aeruginosa, MRSA, CRE, C. auris and C. difficile) compared to only P. aeruginosa and C. auris after 8 seconds of exposure. The optimal exposure time for this device is determined to be at least 8 seconds to achieve, on average, a ≥ 3 log10 reduction. To achieve ≥ 4 log10 reduction on average, then at least 10 seconds of exposure should be applied.
The concentration of ozone was measured at 3 feet above the device to ensure the safety of laboratory personnel. Because ozone concentrations and UV-C wavelength were not measured at the surface of the device, these values cannot be verified, which is a limitation of this study. In addition, this study was performed under controlled conditions in a laboratory setting. Therefore, our results may not be generalizable to the real-world environment. Field studies evaluating the efficacy and impact of shoe disinfection on floor transmission are needed.
The log10 reductions reported in this study appears to be due to the combination of UV-C irradiation and ozone exerting a synergistic microbicidal effect. This study underscores the importance of the exposure time when considering UV-C irradiation and ozone for disinfecting surfaces. We found that increasing the exposure time to 10 seconds ensured > 3 log10 reductions for all pathogens tested except for Aspergillus spp.
Acknowledgements
This study was performed by NSF International in Ann Arbor, MI. Thank you to NSF Microbiology lab for conducting the testing and providing audited test results.
References
(1) Paduszyńska K., Rucińska L.G., Pomorski L. Physician as an infective vector at a department of surgery. Pol Przegl Chir. 2015 Feb 3;86(11):511-7. doi: 10.2478/pjs-2014-0091.
(2) N., Boswell, T. Non-slip socks: a potential reservoir for transmitting multidrug-resistant organisms in hospitals? J Hosp Infec 2016; 94:273-275.
(3) Rashid T., Vonville H., Hasan I., Garey K.W. Mechanisms for floor surfaces or environmental ground contamination to cause human infection: a systematic review. Epidemiol Infect. 2017 Jan; 145(2):347-357.
(4) Rashid T., Vonville H., Hasan I., Garey K.W. Shoe soles as a potential vector for pathogen transmission: a systematic review. J. Applied Microbiol. 2016 Nov;121(5):1223-1231. doi: 10.1111/jam.13250.
(5) Sehulster L.M., Chinn R.Y.W, Arduino M.J, Carpenter J., Donlan R., Ashford D., Besser R., Fields B., McNeil M.M., Whitney C., Wong S., Juranek D., Cleveland J. Guidelines for environmental infection control in health-care facilities. Recommendations from CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). Chicago IL; American Society for Healthcare Engineering/American Hospital Association; 2004. Retrieved from https://www.cdc.gov/infectioncontrol/guidelines/environmental/index.html.
(6) Rutala W.A., Weber D.J. Disinfectants used for environmental disinfection and new room disinfection technology. Am J Infect Control 2013; 41(Suppl):S36-41.
(7) Buonanno M., Ponnaiya, B., Welch D., Stanislauskas M., Randers-Pehrson G., Smilenov L., Lowy F. D., Owensb D.M., Brennera D. J., Germicidal Efficacy and Mammalian Skin Safety of 222-nm UV Light. Radiation Research 2017; 187:493–501.
(8) Rutala W.A., Gergen M.F., Tande B.M., Weber D.J. Room decontamination using an ultraviolet-C device with short ultraviolet exposure time. Infect Control Hosp Epidemiol. 2014 Aug;35(8): 1070-2. doi: 10.1086/677149.
(9) Roushdy M.M., Abdel-Shakour E.H. and Abdel-Ghany T.M. Sporicidal Effect of Ozone on Fungal and Bacterial Spores in Water Disinfection. J of Am Science. 2011; 7(1).
(10) Rashid T., Poblete K., Amadio J., Hasan I., Begum K., Alam M.J., Garey K.W. Evaluation of a shoe sole UVC device to reduce pathogen colonization on floors, surfaces and patients. J. Hosp Infec 2018 Jan; 98(1):96-101. doi: 10.1016/j.jhin.2017.10.011.
(11) Liu J., Zhou L., Chen J., Mao W., Li W., Hu W., Wang S., Wang M. Role of Ozone in UV-C Disinfection, Demonstrated by Comparison between Wild-Type and Mutant Conidia of Aspergillus niger. Photochemistry and Protobiology. 2013; 90(3):615-621. doi: 10.1111/php.12217.
(12) Begum M., Hocking A.D., Miskelly D. Inactivation of food spoilage fungi by ultra violet (UVC) irradiation. Int J Food Microbiol. 2009 Jan 31;129(1):74-7. doi: 10.1016/j.ijfoodmicro.2008.11.020.







