



Peer Reviewed
Affiliation: The University of Arizona, Mel and Enid Zuckerman College of Public Health, Environment, Exposure Science and Risk Assessment Center (www.esrac.arizona.edu), Tucson, AZ, USA.
Disclosures: Dr. Reynolds received funding from Medentech to evaluate third-party data from two separate laboratories and summarize the results for this publication. Data were not produced from the author’s own laboratory but were independently validated by the third-party laboratories as accurate when provided to Dr. Reynolds.
Abstract
Environmental surfaces are frequently contaminated with microbes and contribute to the spread of infectious agents. Despite effective surface disinfectants, maintaining hygienic surfaces is difficult due to commonly touched surfaces that are readily recontaminated. Recent innovations in infection control include continuously active disinfectants that kill microbes and prevent the growth of harmful biofilms over extended periods. Such discoveries are a game-changer in the field of infection prevention.
Background/Introduction
Contaminated surfaces (i.e., fomites) are known to contribute to household and community disease transmission as well as the spread of healthcare-associated infections. (Reynolds, Beamer, Plotkin, Sifuentes, Koenig, & Gerba, 2016; Reynolds & Gerba, 2017; Weber, Anderson, & Rutala, 2013) Microbial tracer studies have shown that spread of microbes is extensive in indoor environments, involving a wide range of surfaces and increasing the risk of infection. (Kurgat, Sexton, Garavito, Reynolds, Contreras, Gerba, & Reynolds, 2019; Reynolds, Sexton, Pivo, Humphrey, Leslie, & Gerba, 2019; Sifuentes, Koenig, Phillips, Reynolds, & Gerba, 2014) One study estimated that in less than four hours, contaminated hands from a single sick individual can contaminate 51% of commonly touched surfaces in an office environment. (Beamer, Plotkin, Gerba, Sifuentes, Koenig, & Reynolds, 2015) Pathogens may survive on surfaces for days to weeks, further increasing the probability of exposure and adverse health outcomes. (Boone & Gerba, 2007; Kampf, 2020).
The survival and persistence of pathogenic microbes are enhanced by the formation of wet and dry surface biofilms. A biofilm is a structured collection of microbes (i.e., bacteria, fungi, algae, yeast, and protozoa) embedded in a self-produced, extracellular polymeric substance (EPS), or slime layer. Pathogen association with biofilm communities is a key survival factor in the environment that provides protection from biocides and enhances growth opportunities. As biofilms mature, populations of cells may be firmly or weakly attached, allowing the biofilm to persist over time and to break off and be dispersed in the environment. Microbes, including multidrug-resistant organisms (MDRO), protected within biofilms are common and can persist on dry surfaces for months or longer. (Hu, Johani, Gosbell, Jacombs, Almatroudi, Whiteley…& Vickery, 2015) Several studies have shown that viable Staphylococcus aureus cells associated with dry surface biofilms were recoverable and capable of regrowth even after multiple applications with bleach (sodium hypochlorite) based disinfectants. (Almatroudi, Hu, Deva, Gosbell, Jacombs, Jensen,… & Vickery, 2015; Hu et al., 2015) Given that persistent populations readily regrow and disinfectants have reduced efficacy in the presence of microbial biofilms, proactive prevention of the formation of these complex communities is warranted. (Abdallah, Benoliel, Drider, Dhulster, & Chihib, 2014)
Surface cleaning, disinfecting, and other hygiene protocols are highly effective at removing and killing pathogens when applied properly. However, many factors limit traditional cleaning and disinfecting efficacy including product and personnel issues (e.g., personnel shortages, training deficiencies). (Boyce, 2016) Common problems include widespread contamination, frequent recontamination, organic load interferences, missing contaminated surfaces during cleaning, poor adherence to manufacturer contact time guidelines, and more, which can increase pathogen exposure potentials.
Innovations in surface disinfection products include chemistries that provide a residual effect where microbial concentrations are reduced or inhibited from growing on treated surfaces. Although little research has been published on the use and efficacy of residual, continuously active disinfectants (CAD), several studies have shown that antimicrobial surfaces provide supplemental support for surface decontamination and biofilm inhibition between routine disinfection practices.
Studies evaluating the long-term efficacy of CAD and residual hand sanitizers have shown sustained benefits over time. (Boyce, Havill, Guercia, Schweon, & Moore, 2014; Tamimi, Carlino, & Gerba, 2014; Wilson, Reynolds, Jaykus, Escudero-Abarca, & Gerba, 2019) One study found that the use of a quaternary ammonium organosilane compound bound to surfaces and reduced the average bacterial counts by >99% for at least 8 weeks. (Tamimi et al., 2014) Ellingson, Pogreba-Brown, Gerba & Elliott (2020) evaluated the impact of an antimicrobial surface coating on the reduction of bacterial colony-forming units and hospital HAIs. In multiple hospital site evaluations, bacterial counts on treated surfaces were reduced by 75-79%, relating to a 36% decline in pooled HAIs in treated compared to control units. (Ellingson et al., 2020)
Most residual disinfectant formulations have included quaternary ammonium compounds. (Brady, Lisay, Yurkovetskiy, & Sawan, 2003) One preliminary study found a mixed quat CAD maintained antimicrobial activity in five minutes 24 hours post-application. Mean log10 reductions, however, varied depending on the pathogen type, ranging from 2 logs with carbapenem-resistant (CRE) Klebsiella pneumoniae and CRE Enterobacter to over 4 logs with S. aureus, vancomycin-resistant Enterococcus (VRE), and other clinically relevant pathogens. (Rutala, Gergen, Sickbert-Bennett, Anderson, & Weber, 2019)
Here we discuss the usefulness of a sodium dichloroisocyanurate (NaDCC) CAD in the form of a fast-dissolving effervescent tablet. (Klorkleen 2 tablets; Medentech, Clonard, Ireland) Once dissolved in water, the hypochlorous acid (HOCl) biocide is released. Studies comparing bleach (sodium hypochlorite; NaClO) with NaDCC generally found the latter to be safer to use and store, more effective against a broader spectrum of pathogens and in the presence of soil and biofilm, and less corrosive. (Bloomfield & Uso, 1985; Coates, 1985) Studies have also found that NaClO did not prevent the regrowth of S. aureus from dry biofilms. (Almatroudi, Gosbell, Hu, Jensen, Esedido, Tahir, …&Vickery, 2016)
Klorkleen 2 (KK2) is EPA registered with claims against a wide variety of bacteria, viruses, fungi, spores, and biofilm pathogens (EPA 71847-7). The goal of this paper is to summarize proof of efficacy data for KK2 as an antibacterial surface coating as evaluated by two third-party U.S. laboratories, one evaluating surface antimicrobial efficacy and the other evaluating biofilm inhibition. Results were submitted to the sponsoring agent and verified to this author independently.
Materials & Methods
Surface antimicrobial testing. Microchem Laboratory (Round Rock, TX), an EPA and FDA GLP-compliant testing organization, adapted the Japanese Industrial Standard (JIS) Z 2801 to evaluate the antibacterial efficacy of the KK2 surface coating on non-porous surfaces over a 24-hour contact time. Although JIS Z2801 is a Japanese guideline, it has become the industry standard in the United States and was confirmed by the International Organization for Standardization (ISO 22196) for the measurement of antibacterial activity of antibacterial treated plastics and other non-porous surfaces by evaluating the prevention of bacterial growth or reduction of surface microbial concentrations. (International Organization for Standardization Technical Committee ISO/TC 61, 2011) The in vitro test has been validated in a round-robin and found to be reliable for testing biocidal activity of antimicrobial surface coatings, provided experimental design factors, such as test organisms, growth medium, cell numbers, and time, are consistently controlled. (Wiegand, Völpel, Ewald, Remesch, Kuever, Bauer, J., … & Bossert, 2018)
Test product. A sodium dichloroisocyanurate (NaDCC) active (Klorkeen 2 High Foam Disinfectant Effervescent Tablet; Medentech, Clonard, Ireland). Biocide tablets were dissolved in 256.6 ml of sterile reverse osmosis treated water and stirred for 15-30 min at ambient room temperature (range=59oF to 86oF) to achieve a final concentration of 4,000 ppm available chlorine.
Bacterial pathogens tested. S. aureus (ATCC 6538), a Gram-positive, spherical-shaped, facultative anaerobe, and Clostridium difficile (ATCC 43598), a Gram-positive, rod-shaped, endospore generating, obligate anaerobe were used in the surface challenge studies. C. difficile endospores serve as a benchmark for disinfectant efficacy due to their persistence in the environment and inherent resistance to antimicrobial agents. C. difficile spores were prepared and purified from vegetative cells using the US EPA SOP MB-28 method. (USEPA Office of Pesticide Programs, 2014)
Procedure. As reported by Microchem, test organisms were propagated in a liquid culture medium and suspended in nutrient broth. Carriers were treated with 0.5 mL of a 4,000 ppm solution of the CAD and allowed to air dry for 30 min in a laminar flow hood. Carriers were visibly dry before seeding. Untreated control and treated test surfaces (e.g., acrylic carriers, 50 mm x 50 mm) were inoculated with microbial seeds and covered with a thin, sterile film to facilitate even spreading of the inoculum, reduce evaporation, and ensure optimal contact with the antimicrobial surface.
Time zero samples were immediately eluted using Dey-Engly (D/E) neutralizing broth, diluted, and plated for quantitative analysis. Additional carriers were inoculated, as described above, and allowed to incubate undisturbed in a humidity-controlled environment for 1, 6, and 24 hours at 37oC. After incubation, carriers were eluted with D/E neutralizing broth and quantified via the spread plate method using tryptic soy agar (TSA) or brain heart infusion agar with horse blood and taurocholate (BHIY-HT) media, with 48-72 h incubation at 37oC. The reduction of microorganisms relative to the control surface was calculated to determine percent reduction and log reduction values.
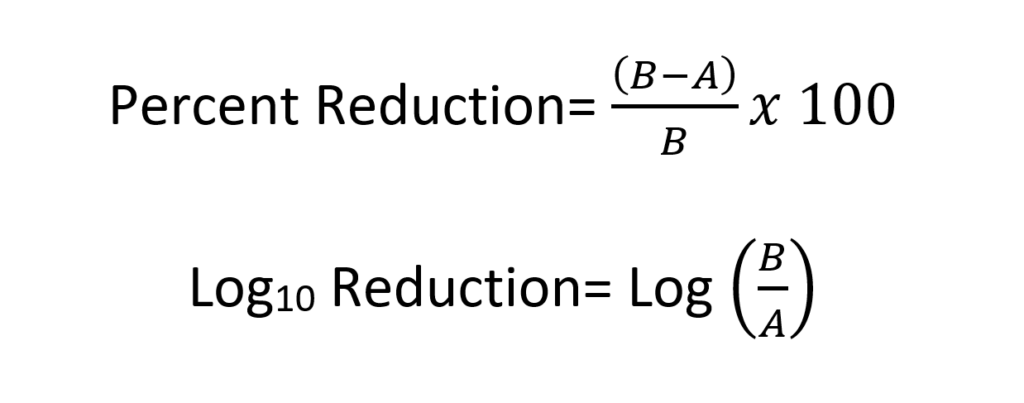
Quality Control. Quality control criteria were developed for studies using the JIS Z 2801 protocol. Specifically, seed bacteria recovered from time zero control samples must be equal to or greater than 1.0 x 104 CFU/cm2 and this level should be similarly maintained over replicate trials. Loss of seed concentration on controls carriers should not be greater than 2 log10. Any bacterial growth measured must be confirmed as representative of the seeded test organism and not some other interfering microbe, negative controls should not test positive for any level of seeded test organism, and a minimum 2 log10, or 99% reduction, relative to control carriers must be observed. Results were calculated as shown below where A = Number of viable test microorganisms on the test carriers after the contact time and B = Number of viable test microorganisms on the control carriers after the contact time.
Biofilm inhibition studies. Supplemental to the CAD surface studies, additional experimental trials were completed to evaluate the inhibition of young biofilms on stainless steel coupons, treated with KK2. These experiments were conducted by an independent laboratory and the results were independently verified (Paul Sturman, Center for Biofilm Engineering, Montana State University).
Test product. A sterile 400 ppm AOAC hard water sample was used to dilute biocides and serve as a negative treatment control. Biocides were prepared as per manufacturer directions by dissolving 4, 3.34 g tablets in 1 quart (0.95 liters) of 400 ppm AOAC hard water to produce 4,306 ppm available chlorine.
Procedure. Stainless steel carriers, with a surface roughness value (Ra) of approximately 21 µIn (or 0.5 µm), were cut from rod stock on a lathe and suspended for 1 hour in the liquid biocide, removed, and air-dried. In these experiments, S. aureus stocks were grown overnight via incubation at 37oC in TSB (tryptic soy broth) growth medium. Carriers were placed into a 12-well microtiter plate and saturated with bacterial stock concentrations of 107 CFU/mL suspended in minimal media. Plates were incubated at room temperature for 24 h to stimulate biofilm production.
Following incubation of biocide-treated carriers with bacterial seed stocks, carriers were removed from the culture plates and gently rinsed to release any planktonic (i.e., unattached) cells. Biofilms were harvested from carriers via a series of vortex and sonication steps at 30 s intervals as per the USEPA standard method for measuring disinfectant efficacy against biofilm growth. (USEPA, 2013) Bacterial concentrations in the biofilm were quantified using a drop plate method and incubation on TSA for 24 h at 36oC. (Naghili, Tajik, Mardani, Razavi Rouhani, Ehsani, & Zare, 2013) Experiments were repeated in triplicate.
In addition, one biofilm coupon per treatment type was evaluated for the presence of adherent cells using fluorescent microscopy and BacLight LIVE/DEAD staining (Cat No. L7012; Thermo Fisher Scientific, Carlsbad, CA).
Results
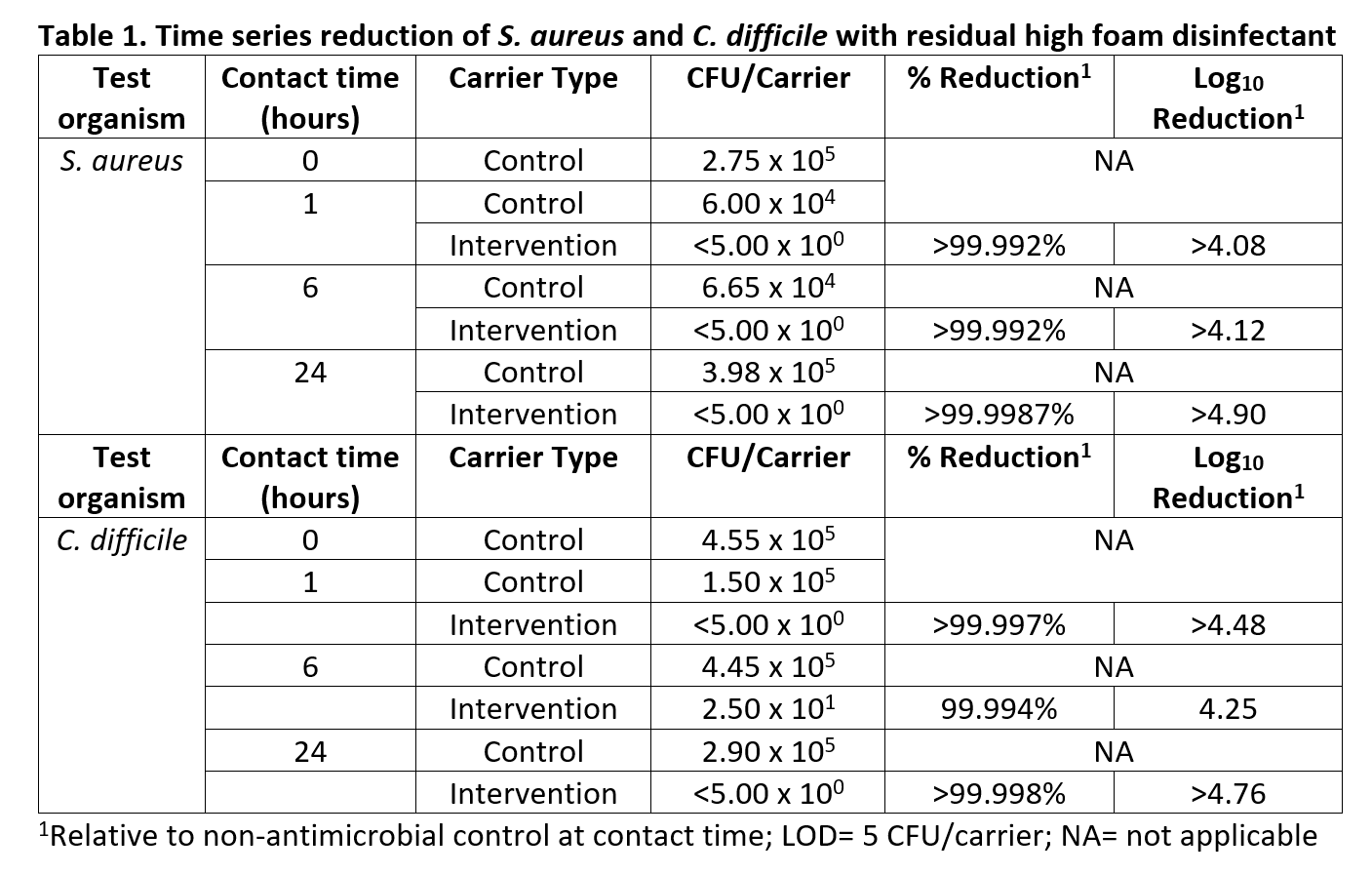
Surface antimicrobial efficacy. Results indicate that bacterial or spore contact with a dry surface-treated 30 min prior with the residual disinfectant, were reduced by a mean of over 4 log10 and be inhibited from growing up to 24 h. (Table 1) Therefore, the product showed sustained residual efficacy. In all three timed scenarios with S. aureus, bacterial concentrations were reduced to below the limit of detection (5 CFU/carrier) from the initial control seed inocula, ranging from 3.98 x 105 to 6.00 x 104. Increasing the initial seed concentration, therefore, might indicate an even greater log reduction efficacy potential for the intervention. Similarly, in two of the three timed scenarios with C. difficile, bacterial concentrations were reduced to below the limit of detection (5 CFU/carrier) from the initial control seed inocula, ranging from 1.50 x 105 to 4.45 x 105. C. difficile represents one of the more difficult surface contaminating pathogens in healthcare environments to inactivate using standard biocides.
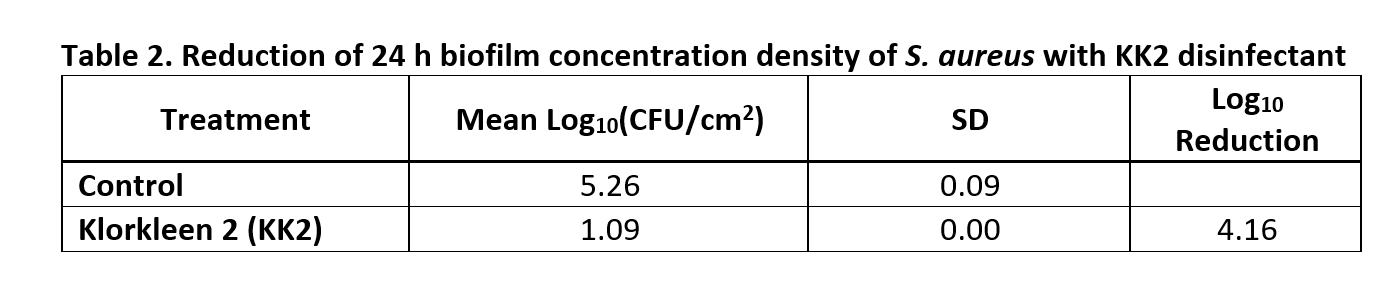
Biofilm inhibition. After biofilm recovery, a mean log10 concentration of 5.26 CFU/cm2 (SD 0.09) of S. aureus seed stocks was measured on the control carriers. The average log10 bacterial concentrations on carriers treated with the biocide intervention were 1.1 (SD 0.00), resulting in an overall log10 reduction of 4.16 (Table 2). Results were consistent, with low standard deviation over replicate trials.
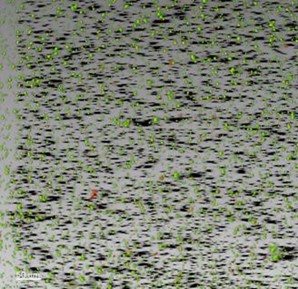
Adherent biofilm experiments showed a discontinuous biofilm with clusters of living cells adhering to the surface of positive control carriers that were mostly green. Treated carriers demonstrated mostly dead (i.e., red) cells, supporting drop plate counts and showing that the biocides reduced bacterial concentrations and biofilm formation. (Figure 1).
 |
 |
|---|
Figure 2: LIVE/DEAD staining of S. aureus biofilm and treated coupons at 250X magnification. Scale bar at the lower left of each picture is 50 µm
Study Limitations
While data from the surface antibacterial efficacy and biofilm inhibition studies showed consistent results, increased replicates across a wider range of variables (i.e., a broader spectrum of pathogens, changing temperature, humidity, and time factors, different textile types) are needed to assess product durability and sustained efficacy. Further, although biofilm adherence experiments supported results of the biofilm density trials and showed a clear and visible reduction in measured LIVE cells, only one replicate experiment was conducted on a young (24 h) biofilm. More replicates are needed to evaluate this observation fully. In addition, more mature biofilms may be more resistant to biocide treatments and should be extensively evaluated.
Given that the limit of detection was reached in four out of the five experimental trials evaluating the disinfectant’s surface antibacterial efficacy, the product’s full potential could not be measured. Future studies should utilize a larger seed concentration so that log reductions can be calculated within the detection limits of the method.
Conclusion and Significance
Numerous studies have found traditional cleaning methods in healthcare environments to be suboptimal and have called for protocol improvements with the consideration of passive, automated antimicrobial interventions. (Dancer, 2014; Reynolds, Sexton, Garavito, Anderson, & Ivaska, 2021) The formation of microbial biofilms on wet and dry surfaces creates additional challenges for contamination control in hospitals, food production, and other critical environments, given increased protection from biocides. (Abdallah et al., 2014) Survival of some organisms ranges from hours to weeks or more, allowing ample time for transmission to susceptible hosts and repeat contamination of surfaces. Interventions that effectively reduce the persistence of pathogens in the environment are expected to have a direct impact on reduced risks of exposure and infection.
While there is not an industry standard for how clean hospital surfaces should be, researchers have proposed an infection control benchmark target of <2.5-5 CFU/cm2 of aerobic colony counts and <1 CFU/cm2 for healthcare-associated pathogens, such as S. aureus and C. difficile. (Dancer, 2014) Although surfaces are routinely contaminated, reductions of bacteria on fomites to <2-log10 have been suggested as appropriate cleanliness goals to achieve acceptable risk targets. (Ryan, Haas, Gurian, Gerba, Panzl, & Rose, 2014) Thus, antimicrobial surfaces with a >2 log10 reduction efficacy may be sufficient to significantly reduce the risk of HAI transmission. (Wilson, Reynolds, Sexton, & Canales, 2018) Indeed, a recent epidemiological study showed a statistically significant reduction in HAIs in two hospital sites resulting from a 75-79% reduction in surface colony counts. (Ellingson et al., 2020) Higher bacterial reduction efficacies have been achieved in the current study with KK2 but application in real-world settings has yet to be evaluated. The next steps are to evaluate product efficacy over time and under more realistic scenarios where surfaces are frequently touched, soil loads accumulate, and microbes are dried onto surfaces as part of the contamination and re-contamination cycle.
This review shows clear benefits of the KK2-CAD technology for the reduction of surface bacteria, including the inherently disinfectant resistant C. difficile spores, and the inhibition of biofilm regrowth. CADs are considered a major discovery in the control of environmental contamination and infection spread. These antimicrobial coatings can be used passively in occupied rooms and continuously supplement manual cleaning to reduce the concentration of environmental pathogens.
Citations
Abdallah, M., Benoliel, C., Drider, D., Dhulster, P., & Chihib, N. E. (2014). Biofilm formation and persistence on abiotic surfaces in the context of food and medical environments. Archives of Microbiology. https://doi.org/10.1007/s00203-014-0983-1
Almatroudi, A., Gosbell, I. B., Hu, H., Jensen, S. O., Espedido, B. A., Tahir, S., … Vickery, K. (2016). Staphylococcus aureus dry-surface biofilms are not killed by sodium hypochlorite: Implications for infection control. Journal of Hospital Infection, 93(3), 263–270. https://doi.org/10.1016/j.jhin.2016.03.020
Almatroudi, Ahmad, Hu, H., Deva, A., Gosbell, I. B., Jacombs, A., Jensen, S. O., … Vickery, K. (2015). A new dry-surface biofilm model: An essential tool for efficacy testing of hospital surface decontamination procedures. Journal of Microbiological Methods, 117. https://doi.org/10.1016/j.mimet.2015.08.003
Beamer, P. I., Plotkin, K. R., Gerba, C. P., Sifuentes, L. Y., Koenig, D. W., & Reynolds, K. A. (2015). Modeling of human viruses on hands and risk of infection in an office workplace using micro-activity data. Journal of Occupational and Environmental Hygiene, 12(4). https://doi.org/10.1080/15459624.2014.974808
Bloomfield, S. F., & Uso, E. E. (1985). The antibacterial properties of sodium hypochlorite and sodium dichloroisocyanurate as hospital disinfectants. Journal of Hospital Infection, 6(1), 20–30. https://doi.org/10.1016/S0195-6701(85)80014-1
Boone, S. A., & Gerba, C. P. (2007). Significance of fomites in the spread of respiratory and enteric viral disease. Applied and Environmental Microbiology, 73(6), 1687–1696. https://doi.org/10.1128/AEM.02051-06
Boyce, J. M. (2016). Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Antimicrobial Resistance and Infection Control. https://doi.org/10.1186/s13756-016-0111-x
Boyce, J. M., Havill, N. L., Guercia, K. A., Schweon, S. J., & Moore, B. A. (2014). Evaluation of two organosilane products for sustained antimicrobial activity on high-touch surfaces in patient rooms. In American Journal of Infection Control (Vol. 42, pp. 326–328). Am J Infect Control. https://doi.org/10.1016/j.ajic.2013.09.009
Brady, M. J., Lisay, C. M., Yurkovetskiy, A. V., & Sawan, S. P. (2003). Persistent silver disinfectant for the environmental control of pathogenic bacteria. American Journal of Infection Control, 31(4), 208–214. https://doi.org/10.1067/mic.2003.23
Coates, D. (1985). A comparison of sodium hypochlorite and sodium dichloroisocyanurate products. Journal of Hospital Infection, 6(1), 31–40. https://doi.org/10.1016/S0195-6701(85)80015-3
Dancer, S. J. (2014). Controlling hospital-acquired infection: Focus on the role of the environment and new technologies for decontamination. Clinical Microbiology Reviews, 27(4). https://doi.org/10.1128/CMR.00020-14
Ellingson, K. D., Pogreba-Brown, K., Gerba, C. P., & Elliott, S. P. (2020). Impact of a Novel Antimicrobial Surface Coating on Health Care-Associated Infections and Environmental Bioburden at 2 Urban Hospitals. Clinical Infectious Diseases, 71(8), 1807–1813. https://doi.org/10.1093/cid/ciz1077
Hu, H., Johani, K., Gosbell, I. B., Jacombs, A. S. W., Almatroudi, A., Whiteley, G. S., … Vickery, K. (2015). Intensive care unit environmental surfaces are contaminated by multidrug-resistant bacteria in biofilms: Combined results of conventional culture, pyrosequencing, scanning electron microscopy, and confocal laser microscopy. Journal of Hospital Infection, 91(1). https://doi.org/10.1016/j.jhin.2015.05.016
International Organization for Standardization Technical Committee ISO/TC 61. (2011). ISO 22196:2011 – Measurement of antibacterial activity on plastics and other non-porous surfaces. Retrieved March 15, 2021, from https://www.iso.org/standard/54431.html
Kampf, G. (2020). How long can nosocomial pathogens survive on textiles? A systematic review. GMS Hygiene and Infection Control, 15, Doc10. https://doi.org/10.3205/dgkh000345
Kurgat, E. K., Sexton, J. D., Garavito, F., Reynolds, A., Contreras, R. D., Gerba, C. P., … Reynolds, K. A. (2019). Impact of a hygiene intervention on virus spread in an office building. International Journal of Hygiene and Environmental Health, 222(3). https://doi.org/10.1016/j.ijheh.2019.01.001
Naghili, H., Tajik, H., Mardani, K., Razavi Rouhani, S. M., Ehsani, A., & Zare, P. (2013). Validation of drop plate technique for bacterial enumeration by parametric and nonparametric tests. Veterinary Research Forum : An International Quarterly Journal, 4(3), 179–183. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/25653794
Reynolds, K.A., Sexton, J. D., Pivo, T., Humphrey, K., Leslie, R. A., & Gerba, C. P. (2019). Microbial transmission in an outpatient clinic and impact of an intervention with an ethanol-based disinfectant. American Journal of Infection Control, 47(2). https://doi.org/10.1016/j.ajic.2018.06.017
Reynolds, Kelly A., Beamer, P. I., Plotkin, K. R., Sifuentes, L. Y., Koenig, D. W., & Gerba, C. P. (2016). The healthy workplace project: Reduced viral exposure in an office setting. Archives of Environmental and Occupational Health, 71(3), 157–162. https://doi.org/10.1080/19338244.2015.1058234
Reynolds, Kelly A., & Gerba, C. P. (2017). Quantifying the impact of hygiene interventions. Household and Personal Care Today, 12(1), 12–13.
Reynolds, Kelly A., Sexton, J. D., Garavito, F., Anderson, B., & Ivaska, J. M. (2021). Impact of a Whole-Room Atomizing Disinfection System on Healthcare Surface Contamination, Pathogen Transfer, and Labor Efficiency. Critical Care Explorations, 1–9. https://doi.org/10.1097/CCE.0000000000000340
Rutala, W. A., Gergen, M. F., Sickbert-Bennett, E. E., Anderson, D. J., & Weber, D. J. (2019). Antimicrobial activity of a continuously active disinfectant against healthcare pathogens. Infection Control and Hospital Epidemiology, 40(11), 1284–1286. https://doi.org/10.1017/ice.2019.260
Ryan, M. O., Haas, C. N., Gurian, P. L., Gerba, C. P., Panzl, B. M., & Rose, J. B. (2014). Application of quantitative microbial risk assessment for selection of microbial reduction targets for hard surface disinfectants. American Journal of Infection Control, 42(11), 1165–1172. https://doi.org/10.1016/j.ajic.2014.07.024
Sifuentes, L. Y., Koenig, D. W., Phillips, R. L., Reynolds, K. A., & Gerba, C. P. (2014). Use of Hygiene Protocols to Control the Spread of Viruses in a Hotel. Food and Environmental Virology, 6(3), 175–181. https://doi.org/10.1007/s12560-014-9158-0
Tamimi, A. H., Maxwell, S., Edmonds, S. L., & Gerba, C. P. (2015). Impact of the use of an alcohol-based hand sanitizer in the home on reduction in probability of infection by respiratory and enteric viruses. Epidemiology and Infection, 143(15), 3335–3341. https://doi.org/10.1017/S0950268815000035
Tamimi, Akrum H., Carlino, S., & Gerba, C. P. (2014). Long-term efficacy of a self-disinfecting coating in an intensive care unit. American Journal of Infection Control, 42(11). https://doi.org/10.1016/j.ajic.2014.07.005
USEPA. (2013). Standard Operating Procedure for Single Tube Method for Measuring Disinfectant Efficacy Against Biofilm Grown in the CDC Biofilm Reactor.
USEPA Office of Pesticide Programs. (2014). Standard Operating Procedure for Production of Spores of Clostridium difficile for Use in the Efficacy Evaluation of Antimicrobial Agents SOP Number: MB-28-04 Title Production of Spores of Clostridium difficile for Use in the Efficacy Evaluation of Antimi. Retrieved from https://www.epa.gov/sites/production/files/2014-12/documents/mb-28-04.pdf
Weber, D. J., Anderson, D., & Rutala, W. A. (2013). The role of the surface environment in healthcare-associated infections. Current Opinion in Infectious Diseases, 26(4), 338–344. https://doi.org/10.1097/QCO.0b013e3283630f04
Wiegand, C., Völpel, A., Ewald, A., Remesch, M., Kuever, J., Bauer, J., … Bossert, J. (2018). Critical physiological factors influencing the outcome of antimicrobial testing according to ISO 22196 / JIS Z 2801. PLOS ONE, 13(3), e0194339. https://doi.org/10.1371/journal.pone.0194339
Wilson, A. M., Reynolds, K. A., Jaykus, L. A., Escudero-Abarca, B., & Gerba, C. P. (2019). Comparison of estimated norovirus infection risk reductions for a single fomite contact scenario with residual and nonresidual hand sanitizers. American Journal of Infection Control, 48(5), 538–544. https://doi.org/10.1016/j.ajic.2019.09.010
Wilson, A. M., Reynolds, K. A., Sexton, J. D., & Canales, R. A. (2018). Modeling Surface Disinfection Needs To Meet Microbial Risk Reduction Targets. Applied and Environmental Microbiology, 84(18), e00709-18. https://doi.org/10.1128/AEM.00709-18
Zheng, Y., & Ayotte, J. D. (2015). At the crossroads: Hazard assessment and reduction of health risks from arsenic in private well waters of the northeastern United States and Atlantic Canada. The Science of the Total Environment, 505, 1237–1247. https://doi.org/10.1016/j.scitotenv.2014.10.089







