



Abstract:
The need for Infection Prevention and Control has become more important than ever, especially in the wake of globalization. In Nigeria the need for Infection Prevention and Control strategies was embraced by different sectors and population in Nigeria in the wake of the 2014 Ebola Viral disease outbreak in Lagos and Rivers states.
The need for concerted efforts that include all and sundry is as important as the need to prevent an occurrence in the first place. It is important to learn from successful programmes (such as Guinea worm and Small Pox eradication) and apply lessons learned to current epidemics that threaten national development and growth.
Main Article:
Introduction
Nigeria occupies a unique position within Africa. Described as the most populous nation in Africa, it is reported to have the largest economy in Africa, although the wealth is unequally distributed amongst the 174 million people1.
Politically, Nigeria has repeatedly led the Economic Community of West African States (ECOWAS) and continues to take the lead in economic growth and development1 with an economy that accounts for 35% of the GDP for sub-Saharan Africa.
In global health, Nigeria will be remembered for contributions to health workforce in terms of manpower.2 Developmental challenges continue to underscore Nigeria’s relevance in terms of global health, despite its large population. In West Africa, Nigeria’s health system is a reference point for neighbouring countries. Its role in drawing attention to the 2014 Ebola Viral Disease (EVD) saga will forever remain on the minds of many West Africans. Nigeria has been fundamental to drawing global attention to the plights of many West African countries that had been besieged with this virulent outbreak. The outbreak was controlled within two months, despite Nigeria’s vast population. This is in large part due to the health professionals at First Consultant Medical Center3 who risked their lives, quarantining the index patient Patrick Sawyer who was on a visit from a neighbouring country, Liberia.
OUTLINE
Infection Prevention/Control & Related Issues in Nigeria
Nigeria has come a long way in preventing/controlling infections; the removal of Nigeria from the list of Polio endemic countries4 recently is one of many reasons to celebrate (the last reported case was in July 2014). As recently as 2012, Nigeria accounted for more than half of all polio cases worldwide5. Nigeria continues to innovate in healthcare, actively participating in efforts to eradicate infectious diseases like Polio, Malaria and Tuberculosis. This is in part responsible for declines in Maternal and Infant Mortality rates.
Like everywhere in the world, Nigeria faces the dangers of infectious diseases: from hospital related infections, to poor vector control, sanitation and refuse disposal challenges, food contamination, unsafe water and sexually transmitted infections (STI). Bacterial infections such as tuberculosis (TB) and meningitis continue to impact Nigeria’s health, while viruses like HIV6 and Hepatitis B (HBV)7 appear to thrive among the population. HBV is reportedly hyperendemic7 in Nigeria and in need of urgent efforts to prevent new infections. The burden of HIV currently stands at 3.3% (3.2 million infected) 6.
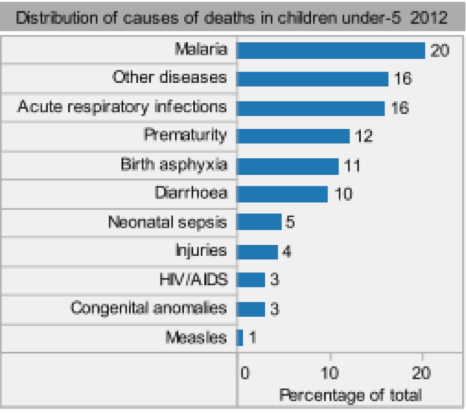
The leading causes of death in Nigeria8 are lower respiratory infections (13.9%), HIV/AIDS (10.4%), malaria (8.7%), diarrhoeal diseases (6.3%), Preterm birth complications (4.7%), birth asphyxia and birth trauma (4.3%), meningitis (3.6%), stroke (3.4%), ischaemic heart disease (2.6%) and protein-energy malnutrition (2.5%). For infants and children, malaria (21%), acute respiratory infections (15%) and diarrhoea (10%) are among leading causes of infant and child morbidity and mortality9.
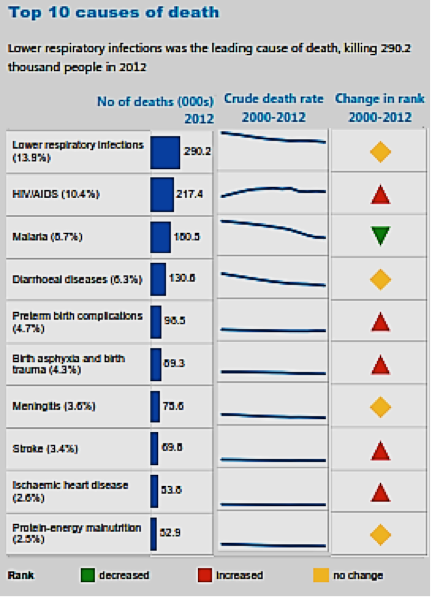
Source: Country statistics (Nigeria) and global health estimates by WHO and UN partners
Global Health Observatory, (http://www.who.int/gho/en/)
Top on the list of dangerous pathogens in Nigeria include Plasmodium, HIV, Mycobacterium Tuberculosis, Vibrio Cholerae, Salmonella, Meningococcal Meningitis, Hepatitis B Virus (HBV) 10 amongst many others.
In this year alone, a “strange” outbreak reported in Ondo state in April 2015 was reportedly believed to be vengeance from “gods” by the locals. Later thought to be contamination from pesticides but eventually confirmed as Ethanol poisoning after post mortem investigations11. Two major Cholera outbreaks were reported between August-October; in the Northeast were the country is presently fighting insurgence in Borno state camps for internally displaced persons (IDP), where more than 1.6 million people affected by the insurgence are sheltered. The official counts as at September 16, according to Médecins Sans Frontières (MSF) 12 were 172 cases and 16 deaths. In October, The other occurred in the Southwest (Ekiti state) in October where 300 students were affected. In the same month (October 30), were reports 13 that refuse took over parts of Ado Ekiti, the state capital while Cerebrospinal Meningitis took a toll on many lives in Northern Nigeria13, 14.
The outbreaks in the IDP camps in Borno were attributed to contamination of water with fecal matter following heavy rainfall that led to overflow of sewage. Poor personal and environmental hygiene and inadequate water supply, worsened by overcrowding and poor environmental conditions, exacerbated the situation. The cases increased sharply and spread to two other contiguous IDP camps in the state. Ten days later, other communities in Maiduguri began to report suspected cases of Cholera14.
2014 EVD outbreak, zero wild Polio case, Cholera outbreaks: What we are learning about Infection Prevention and Control
Community mobilization and involvement! From case monitoring and reporting to contact tracing, one lesson stands out: community involvement is a necessary and important aspect of infection prevention and control. The EVD episode highlighted the need for concerted efforts: all hands must be on deck if progress is to be made. From the health workforce to media and entertainment industries, the marketplace and more, the efforts must be multi-sectorial and multidisciplinary in nature. In other words, there must be a public health approach to get successful public health outcomes. Community involvement cannot be over emphasized, as is evident in the role it played in the fight against polio.
Okwor et al15 suggests there were improvements in actions by all stakeholders during the Nigeria EVD outbreak. The evidence was in a ‘call to action’ for adoption of the Chennai declaration in combating the spread of hospital-acquired infections and in strict adherence to the National Institute for Health and Care Excellence (NICE) quality standards of infection prevention and control and to WHO guidelines. According to Okwor et al15, such policy adoptions illustrated that the outbreak of Ebola had successfully influenced the Nigerian Government, non-governmental organisations, the media, and communities to take infection prevention and control issues seriously.
Government efforts that support infection prevention and control have additionally included the so-called “war” on fake and sub-standard drugs and massive public enlightenment campaigns on health promoting behaviours (proper hand washing and use of hand sanitizers). Additionally, programs have been in place to educate citizens on the authentication of drugs/medicines, policy formulation and enforcement on drug sales, distribution of drugs and drug products and recently, the ban on the import of frozen livestock (poultry).



Media and Community mobilization for Infection (HIV and TB) Prevention and Control in Southwest Nigeria. Courtesy Journalists Against AIDS (JAAIDS) Nigeria and American Jewish World Service (AJWS).
CONCLUSION
To address more comprehensive food and drug regulation, the war on fake and adulterated drugs (to address drug resistance including antibiotics resistance, etc.), has been addressed to a large extent by the National Agency for Food and Drug Administration and Control. Continuous and evolving efforts to implement programs are important to their success.
An adequate supply of safe water and enforcement of sanitation by the government, in partnership with the private sector, must be ensured for the nation of Nigeria. The adequate supply of safe water has far-reaching benefits for sanitation and prevention of water-borne diseases.
Sanitation has been addressed in few states, such as Lagos and Cross River, but a lot still needs be done. This is especially important in rural communities. In some states, mandatory environmental sanitation exercise is observed once every month for all, and every week for market and related places, with strict punishment for non-compliance. This best practice should be extended to all 36 states and the Federal Capital Territory (FCT), Abuja.
There is a need to intensify campaigns that promote ideal behaviours, such as proper hand washing practices, proper disposal of waste/refuse, policy implementation and enforcement/monitoring of workers’ compliance to IPC practices, health education (including media and community mobilization targeting market and community associations) and school health education on IPC.
Another noteworthy point is in reporting disease incidences and outbreaks. The time lag between the start of the Ebola outbreak in West Africa and the international response took several months. A similar trend is evident in the response time to address both Cholera and Meningitis outbreaks in Nigeria this year. Systems should be put in place to promote prompt reporting of future outbreaks.
References:
1. International Monetary Fund: Nigeria 2014 article IV Consultation—Staff Report; Press release and statement by the Executive Director for Nigeria. IMF Country Report No. 15/84, pp 1-13
2. Paula O’Brien and Lawrence O. Gostin: Health Worker Shortages and Inequalities: The Reform of United States Policy; GLOBAL HEALTH GOVERNANCE, VOLUME II, NO. 2 (FALL 2008/SPRING 2009), http://www.ghgj.org
3. The Vanguard (2014); http://www.vanguardngr.com/2014/10/ebola-first-consultant-indicts-liberian-ambassador/; accessed on Nov 14, 2015
4. World Health Organization (WHO) 2015: WHO Removes Nigeria from Polio-Endemic List; accessed at http://www.who.int/mediacentre/news/releases/2015/nigeria-polio/en/; Nov 12, 2015
5. WHO 2015: WHO Removes Nigeria from Polio-Endemic List; accessed at http://www.who.int/mediacentre/news/releases/2015/nigeria-polio/en/
6. Bashorun A , Nguku P, Kawu I, Ngige E, Ogundiran A, Sabitu K, Nasidi A and Nsubuga P, (2014): Pan Afr Med J. 2014; A description of HIV prevalence trends in Nigeria from 2001 to 2010: what is the progress, where is the problem? 18(Suppl 1): 3. Published online 2014 Jul 21. doi: 10.11694/pamj.supp.2014.18.1.4608, PMCID: PMC4199354, accessed at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4199354/pdf/PAMJ-SUPP-18-1-03.pdf
7. BM Musa, S Bussell1 , MM Borodo, AA Samaila, OL Femi (2015): Prevalence of hepatitis B virus infection in Nigeria, 2000-2013: A systematic review and meta-analysis, accessed at http://www.njcponline.com on Saturday, November 14, 2015, IP: 169.159.97.127
8. WHO (2015): Nigeria, WHO Statistical Profile; Country statistics and global health estimates by WHO and UN partners, Global Health Observatory, (http://www.who.int/gho/en/), January 2015;
9. WHO (2015): Country Statistics and Global Health Estimates by WHO and UN partners (http://who.int/gho/mortality_burden_disease/en/). Assessed November 13, 2015
10. Institute of Health Metrics and Evaluation: Global Burden of Disease. Accessed at http://vizhub.healthdata.org/gbd-compare/
11. Premium Times (2015): Nigerian govt. says Ondo strange disease under control, blames “methanol poisoning;” http://www.premiumtimesng.com/news/headlines/181774-nigerian-govt-says-ondo-strange-disease-under-control-blames-methanol-poisoning.html
12. Medecins Sans Frontieres (MSF): http://www.msf.org/article/nigeria-cholera-spreads-displaced-persons-camps-borno-state. Assessed on November 12, 2015
13. Daily Times: http://dailytimes.com.ng/cholera-epidemic-looms-in-ekiti-as-300-fgc-students-are-hospitalised/;
14. Nigerian Pilot (2015): Cholera outbreak hits FG College in Ekiti, 300 students affected – http://nigerianpilot.com/cholera-outbreak-hits-fg-college-in-ekiti-300-students-affected/
15. WHO 2015: Highly contagious meningitis outbreaks continue in African countries; http://www.afro.who.int/en/media-centre/afro-feature/item/7579-highly-contagious-meningitis-outbreaks-continue-in-african-countries.html. Assessed on November 12, 2015.
Article Revised: November 17, 2015 for readablity







