


Abstract:
Despite being preventable in most cases, surgical site infections still occur following 5% of all surgeries in Europe and North America. At the Infection Prevention and Control Conference (Knowlex) held in London on February 23, 2016, Pauline Harrington, a surgical site infection surveillance manager presented the findings from a national surveillance program in the UK monitoring surgical site infections (SSIs). Implementation of surveillance programs and the real time identification of outliers can greatly improve patient outcomes on a national level. Through reduction of SSIs through surveillance, more resources are available to allocate toward caring for primary injuries.
Main Article:
Surgical Site Infections (SSIs) represent one-fifth of all healthcare acquired infections (HAIs) in both North America (20%) and Europe (17%) (1). Despite strategies to reduce the incidence of surgical site infections, 5% of all surgery patients still develop infections (2); this equates to almost 500,000 SSI’s per year(2)! The development of SSIs creates an enormous burden for hospitals. Extended illness, long-term disability, avoidable death and increased antibiotic consumption are estimated to cost Europe almost 7 billion pounds per year.
Surveillance
Public Health England began a national surveillance program of National Health Service (NHS) England in 1997 to monitor SSIs. Three hundred seventy-one hospitals were monitored, and over 102,496 cases were monitored over the period between 2014 and 2015 (3). Patients were monitored for 30 days following surgery, as infections occurring outside of this timeframe are considered to be secondary to SSI. Monitoring was performed on inpatients, and also included post-discharge surveillance through hospital readmission, outpatient and community visits and patient reporting surveys. Two types of SSI were monitored: superficial incisional SSI involves only skin or subcutaneous tissue; while deep incisional SSI involves fascial or muscle layers (4).
Quality Assurance
To ensure high quality data was being reported for the surveillance study, extensive training for healthcare workers to act as surveillance personnel was enlisted. While nurses compromised 79% of the surveillance staff, other infection control personnel, like doctors and healthcare administrators were also included. Continuous support was provided to personnel to resolve clinical queries, and continuous monitoring of data was implemented to improve accuracy of data. Unfortunately, SSI surveillance training was limited for surgical teams, as their compliance was much lower.
In such a large surveillance study, the methodology needs to be explicitly defined. There can be great heterogeneity among hospitals, despite the development of the same SSIs among different patients. These considerations included training to standardize the interpretation of similar case definitions, the high/low risk procedures included, the differences in compliance to standards of care and the length of patient stay. Other factors, which varied from site to site, but were objectively reported, included patient demographics, and funding/staffing support available for patient care.
Results
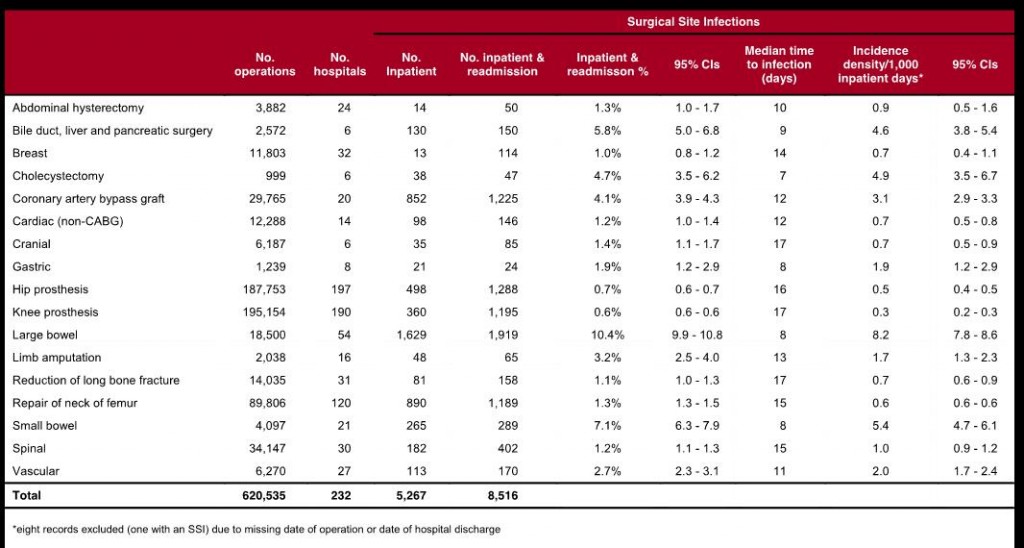
Between 2010 and 2015, 8,516 SSIs developed out of a total 620,535 surgical procedures (1.4% SSI rate). The highest incidence of SSI was seen in large bowel surgery (10.4%), whereas the lowest incidence of SSI was associated with hip and knee prosthesis (0.7% and 0.6%, respectively) (3). Most SSIs were detected through readmissions following short hospital stays, and were found to be fairly infrequent among surgical patients that required longer post-operative hospital stays (Table 1).
Table 1: SSI incidence by surgical category, NHS hospitals in England, April 2010 to March 2015
For the majority of orthopaedic surgeries, the proportion of SSI saw a modest decrease per year, but given the relative infrequency of SSIs already, modest changes may reflect annual fluctuations, rather than a trend.
Of the two types of infection, superficial incision infections were reported to be 28.0% in hip prosthesis to 71.4% in small bowel surgery (3). This was attributed to post-operative hospital stay duration. Conversely, deep wound infections were increased in patients with relatively shorter post-operative hospital stays, and were typically detected during patient readmission (3).
The Culprits
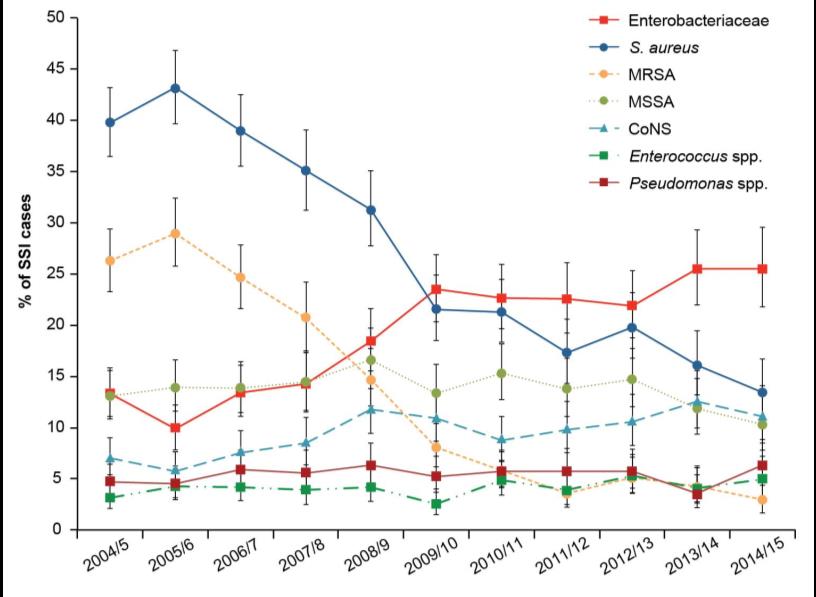
The majority of surgical site infections were caused by Staphylococcus aureus. In orthopaedic surgeries, S. aureus is responsible for more than 36% of SSI. Due to antibiotic stewardship, among other factors, the proportion of methicillin resistant S. aureus (MRSA) infections decreased from 25% of SSIs in 2006/2007 to just 3% of SSI in 2014/2015. As a result, the proportion of Enterobacteriaceae SSIs increased in the same period and was predominantly associated with large bowel surgery (Figure 2).
Figure 2: Trends in key micro-organisms reported as causing inpatient SSIs, all surgical categories
Outlier Identification
Outliers are inevitable. In performing a large surveillance study, hospitals that were experiencing a higher than normal number of infections (more infections than 95% of other sites), could be identified and notified of an increase in the number of SSI. Hospitals were then required to acknowledge the increase, and put forth a plan on how to reduce the SSI frequency. Eight sites were identified as high outliers that needed to address their infection control standards.
Following this study, it was found that the hospitals and trusts that constituted the low outliers all had a few similarities in their standards of patient care. These hospitals all employed a multidisciplinary approach to reducing infection, emphasizing coordination between surgical and post-operative health teams. Monitoring by external bodies (such as Public Health England) was also found to be effective.
Conclusion:
Ongoing surveillance studies are important for the creation of meaningful data. Establishing benchmarks using a diverse data set creates a baseline to which hospitals and trusts can either strive to achieve or improve upon. Comprehensive surveillance studies, coupled with outlier identification, can reduce the number of adverse events by providing continuous monitoring and response from surveillance teams.
Slides: https://media.wix.com/ugd/f70a7d_f134dc1f89f547a18e54628c3c2ee507.pdf
About Knowlex:
Knowlex, shorthand for ‘Knowledge Exchange’, is a new organisation that has been set up with the ambition of disseminating information on research and innovative practice to help healthcare professionals in their working lives.
Upcoming Conference:
Tuesday 6th September 2016 RNCM Manchester, UK
European City of Science 2016
In light of estimates that the total cost of AMR to healthcare systems within OECD countries will reach £1.9 trillion by 2050, on 8th September 2016, Knowlex will welcome more than 350 healthcare professionals to Manchester, European City of Science, for Infection Prevention & control 2016.
Conference Website: http://www.infectioncontrolmanchester2016.co.uk/
References:
- Leaper DJ. Surgical-Site Infection. Br J Surg. John Wiley & Sons, Ltd.; 2010 Nov; 97(11):1601–2.
- Anderson DJ. Surgical Site Infections. Infect Dis Clin North Am. 2011;25(1):135–53.
- Public Health England. Surveillance of surgical site infections in NHS hospitals in England: 2014 to 2015. London; 2015. Available from: https://www.gov.uk/government/publications/surgical-site-infections-ssi-surveillance-nhs-hospitals-in-england
- European Centre for Disease Control. Surveillance of surgical site infections in European hospitals – HAISSI protocol. Version 1.02. Stockholm; 2012. Available from: http://ecdc.europa.eu/en/publications/Publications/120215_TED_SSI_protocol.pdf







