



Disclosure statement: InfectionControl.tips declare no conflict of interest with the following critical evaluation and research. No funds or influence were provided to InfectionControl.tips by any parties.
Abstract
Background
Numerous articles have highlighted the role of waterborne nosocomial/Health-Care Associated Infections (HAIs) in terms of morbidity and mortality among immuno-compromised patients and the efficacy of Point of Use Filters (PoUF) for their control. Since their first large-scale use in Europe (France) for controlling the Legionellosis outbreak in the Georges Pompidou hospital in Paris (winter 2000/2001) with the necessity to replace each filter twice a week, progresses have been made for extending the life period to 31 days. To address this issue, a self-cleaning mechanism has been developed which introduces turbulent flow during filtration to keep particulates from becoming fully trapped on the membrane.
Significance
This allows longer extended use as confirmed through Heterotrophic Plate Count (HPC) evaluations as described in this article. The reduction of Legionella using 62-days filters were observed up to 3 and 4 months after installation. This success reflects an important cost factor reduction linked to the method of water-borne infection control.
Main Article
Introduction
Since the first paper by Anaissie et al. (2002), many experimental studies and outbreaks investigations around the world have shown that immunocompromised patients may suffer of waterborne HAIs especially in ICUs. These infections are linked to a large variety of microorganisms including Legionella, Gram negative bacteria, Aspergillus, et (Exner et al, 2005) The largest part of microorganisms present in water pipes lives within the biofilm extremely difficult to eradicate since established, including protozoa which are very resistant to disinfectants, including e.g. Acanthamoeba and Vermamoeba (Fouque et al, 2015). Thus, one easy way to control their presence in the water is to use disposable water filters at the tap, called point of use filters (PoUF) . This was first developed in France during the famous Legionellosis outbreak in the European Hospital Georges Pompidou in Paris in 2000 (Weber, 2001) . At this period, the filters using membranes rated at 0.2 micron were used for 2 or 3 days according to Hartemann and Hautemaniere (2011). The cost of their use was elevated and too high for permanent use, but required during a crisis. Since this first episode, the period of use has been extended until 31 days but due to the possible presence of organic matter in the water circulating in more or less corroded pipes, clogging could occur on the filter membrane ( Sheffer et al- 2005). Thus, the limitation to this extended life time lies with their ability to handle large volumes of water without a significant reduction in flow due to clogging before replacement becomes necessary.
To address this issue, Aqua-Tools has developed a new technology for water filtration, trade marked as the Bubl’Air Wash™ technology that limits the clogging on the surface of the filter. Prevention of the clogging on the filtrating surface of hollow-tubular filtration membranes by a self-cleaning mechanism through turbulent flow in the carter during filtration. This technology could allow a limitation of the clogging on the filters, as a consequence these filters are hoped to have a longer life use with a good flow and reliable bacteriological resuts at the outlet.
Material / Methods
Filters
In this experiment, FILT’RAY 2G Point-of-Use filters using sterilizing-grade tubular membranes with a fixed 0.1 µm pore size ensuring high performance filtration and the so called Bubl’Air Wash™ technology allowing inside the carter a self-cleaning mechanism linked to a turbulent flow. The 31 & 62 days and 3 & 4 months PoUFs are intended for rinsing medical devices (bacteriologically controlled water) and serve for the personal hygiene of the patients as well as washing surgeon’s hand. They are tools for environmental management and are used to protect patients and/or residents against waterborne microorganisms (Figure 1).
Laboratory-based microbiological challenges were performed according to the American Standard Test Method (ATSM) F838.
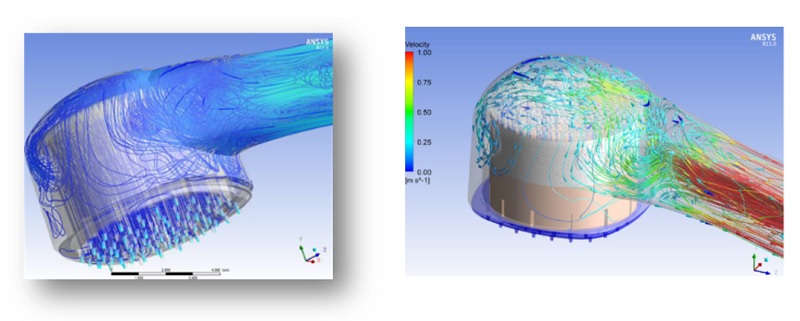 FIGURE 1: FILT’RAY 2G Disposable Water Filters, BuBl’Air Wash TM
FIGURE 1: FILT’RAY 2G Disposable Water Filters, BuBl’Air Wash TM
Two fields evaluations of a new extended life of duration that includes the Bubl’Air Wash™ technology have been performed in the US and in France by two independent research teams. Experiment 1 was performed on 62 day filters has been performedby the Special Pathogens Laboratory USA on shower and faucet filters for 12 weeks (84 days) in real use conditions to evaluate the efficacy for removal of Legionella and Heterotrophic Plate Count (Stout et al 2017). 500 mL hot water samples were collected from each outlet weekly. Phase 1 baseline samples were collected prior to filters placements (120 faucets samples, 10 faucets over 12 weeks) and 120 shower samples (10 shovers outlets over 12 weeks) and the same protocol has been followed after filter placement (Phase 2). Total Heterotrophic Plate Count (HPC) and Legionella were monitored in the laboratory according to the standard methods (Baron et al-2014). For statistical tests, variance analysis and Student t tests were used for comparing the results.
Experiment 2 utilized 3 and 4 months filters in a health care facility by the Infection Prevention & Control Department of Hospices Civils de Lyon, France. Twelve shower filters were installed in the cardiology department and the Legionella retention was measured along this period in comparison with 12 control showers, during 12 weeks (6 showers) and 16 weeks (6 other showers). 500 mL hot water samples, control and initial value before fiter placement and at the end of the test period (12 & 16 weeks respectively) were analyzed for Legionella enumeration according to the french standard AFNOR NF T90-431 and the results treated with the aid of the same statistical tests (Cassier & al-2017).
Results
In the first assay preformed, there was no significant difference in L. pneumophila between test (with filter) and control fixtures. During week 1 to 12 after the installation of the filter, L. pneumophila remained non-detectable in both the filtered faucets and showers. During the same period, L. pneumophila was detected in all control fixtures at a concentration ranging from 22.6 CFU/ mL to 191.2 CFU/ mL in control showers (Figure 2. Stout et al, 2017).
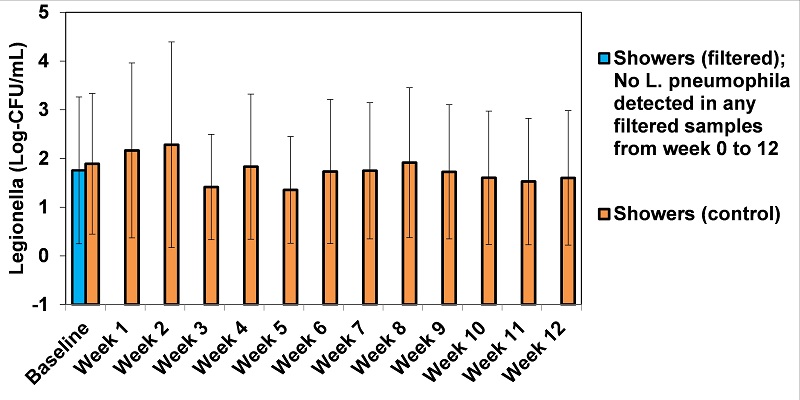
Figure 2. L. pneumophila concentration (Log10-CFU/mL) from all showers with filtered and without (control) point-of-use filters throughout 12 weeks of usage (Stout et al, 2017)
The same results were obtained with the measurement of HPC. At baseline it was no difference in HPC between the test and control fixtures and from week 1 to 12 post the installation of the PoUFs, HPC concentration after filtration ranged from non-detectable to 19.6 CFU/m mL in comparison with a concentration ranging from 9.6 to 27935.6 CFU/m mL in the controls. These results indicate the PoUFs reduced the overall abundance of bacteria in both faucets and showers.
The test of long term efficacy (3 and 4 months of use) of microfilters on Legionella pneumophila, all the 12 tested showers samples grew positive for L.pneumophila (growth range: 630 CFU/ mL -750 CFU/ mL) as well as control showers during the study (growth range: 15-25 CFU/ mL) before the installation of the filters. The difference is not statistically significant and these resuts illustrate the regular contamination of the faucets by Legionella. The difference is dramatically evident after placement of filters: All 6 water samples from 3 months filters and 6/6 samples from 4 months filters were negative for L. pneumophila in the conditions of the study. This demonstrates the ability of theses 3 or 4 months filters to remove) L. pneumophila from the water during the test periods, which can limit the risk of immuno-compromised patient’s contamination.
Discussion
Both assays demonstrated the absence of Legionella contamination at the outlet of the PoUFs filters during the tested periods of 3 and 4 months while obtaining a usable flow rate of filtered water compatible with its use for medical cares or patient’s showering. This performance is achieved during all the test period. The continuous presence of Legionella in the control faucets and showering points during the same period in the hot water networks of theses two different hospital insures this result is not due to an intermittent contamination of the network as described previously by Sheffer et al (2005).
During the assay performed in the hospital, the analysis filtered water samples demonstrates the presence of HPC and the absence of opportunistic pathogens for the patient that would regurlarly shower. This alludes to the possibility of a retro-contamination of the external part of the filter when no specific prevention measures are taken for avoiding this contamination.
Conclusion and Significance
The two studies described above demonstrate the performances of the new extended life PoUFs under real use conditions in removing hazardous microorganismsfor 62 days, 3 and 4 months with the production of usable waterflows. Longer extended duration of use of this innovative generation of disposable PoUFs allows to decrease the amount of labour associated with replacement, and reduced volume of waste. This also reduce the potential burden for the patients when the filters are changed in their rooms. This also leads to a cost reduction while purchasing only one filter in replacement of three or four 31-days filters, which can be as high 35% (Baron et al-2014)
References
Anaissie, E., Penzak, S. and Dignani, C. (2002), The hospital water supply as a source of nosocomial infections. Achives of Internal Medicine, 162,483-92.
Baron, J., Peters, T., Shafer, R. MacMurray, B. and Stout, J.E. (2014). Field evaluation of a new point-of-use faucet filter for preventing exposure to Legionella and other waterborne pathogens in health care facilities. American Journal of Infection Control, 42, 1193-6.
Cassier,P., Coudrais, S., Gardes, S., Gerbier-Colombani, S., Vanhems P. and Raymond, M.(2017). Evaluation of the efficacy of 3 and 4 months of use microfilters on Legionella pneumophila in real life conditions in a healthcare facility. International Legionella Congress. September, Rome
Exner, M., Kramer, A., Lajoie, L., Gebel, J., Engelhart, S. and Hartemann, P. (2005). Prevention and control of health-care associated waterborne infections in health care facilities. American Journal of Infection Control, 33, S26-40.
Fouque. E., Hechard. Y., Hartemann. P., Humeau. P. and Trouilhe M.C.(2015), Sensiyivity of Vermamoeba (Hartmanella) vermiformis cysts to conventional disinfectants and protease. Journal Water & Health,13, 2, 302-310.
Hartemann. P. and Hautemanière. A. (2011). Legionella prevention in France. Bundesgesundsheitblatt. 54, 6, 724-727.
Sheffer. P.J.,Stout. J.E., Wagener. M.M. and Muder R.R. (2005). Efficacy of New point-of -use filter for preventing exposure to Legionella and waterborne bacteria. American Journal of Infection Control, 33, 5, 520-525.
Stout, J.E., Parkinson, J., Betts, S. and Racine, P. (2017). Role of point of use filters in prevention of Legionnaires’ disease: results of two field evaluations of faucet and shower filters. A.W.T. annual convention and exposition, Sept. 13-16.
Weber. W. (2001). Paris’ Pompidou hospital plagued by setbacks. Lancet, 357,9250, 130.







