



Peer Reviewed
Cite as: Morales K, Puri K, Knighton S, Greene C, et al. (2020) Position on Healthcare Client Hand Hygiene. InfectionControl.tips. 7: 1-24
Abstract
Recent public health concerns call for innovative strategies to better protect healthcare clients. Pathogens which can lead to healthcare-associated infections (HAIs) are found on the hands of healthcare workers and clients. Hand hygiene is the most effective and economical behavior to reduce pathogen transmission. Although hand hygiene is frequently mentioned to the public to address community-associated infections, the context rarely addresses the client’s role in HAI prevention.
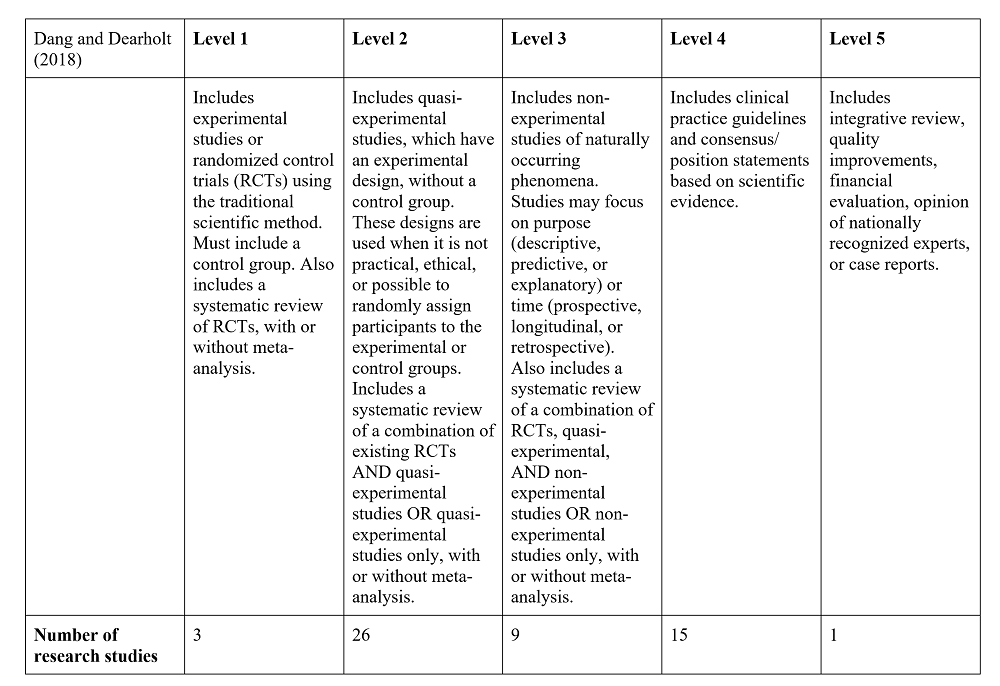
A literature review addressed the following evidence-based practice question: Does the implementation of healthcare client hand hygiene decrease pathogen transmission? Fifty-four studies spanning 17 years (2002-2019) were appraised using Dang and Dearholt’s (2018) five levels of evidence with Level 1 being the most stringent to develop and support our position on client hand hygiene.
Several research studies found clients’ hands become a reservoir and means of transmission if not adequately cleansed. Effective education increased the frequency of client hand hygiene, decreased pathogens found on their hands, and subsequently, decreased HAI rates across healthcare settings. Effective education led to greater client and worker engagement, increased worker hand hygiene adherence, and increased frequency of visitor/family hand hygiene.
We present an evidence-based multimodal strategy that is affordable, practical, effective, acceptable, safe, and equitable.
Key Words
Hand hygiene, patient hand hygiene, client hand hygiene, resident hand hygiene, long-term care, acute-care, healthcare-associated infections
Definitions
Hand hygiene: An inclusive term for the practice of cleansing hands, which includes hand washing, use of alcohol-based handrubs, or disposable wipes. Hand hygiene does not refer to surgical hand antisepsis performed in surgical settings (World Health Organization, WHO, 2009.
Hand hygiene supplies: Includes sinks, alcohol-based handrubs, and disposable wipes.
Healthcare-associated infections (HAIs): Infections acquired while receiving treatment for other conditions within a healthcare setting (Centers for Disease Control, CDC, 2002).
Healthcare client: Recipients of care in any healthcare setting, including inpatient, outpatient, and/or long-term care settings. Referred to as client in this paper. The role of visitor hand hygiene will be addressed in a separate paper.
Healthcare worker: Licensed and unlicensed employees in the healthcare setting, including inpatient, outpatient, and/or long-term care settings. Referred to as worker in this paper.
Introduction
Recent public health concerns such as the coronavirus pandemic and the global threat of pathogens such as Ebola call for innovative strategies to better protect healthcare clients. Harmful bacterial, viral, and fungal pathogens, including multidrug-resistant organisms (MDROs), are found on the hands of healthcare workers and clients. Most of these pathogens can lead to HAIs (Cao et. al, 2016; Mody et al., 2019). Hand hygiene is the most effective and economical behavior to reduce transmission of potentially harmful organisms and subsequent HAIs (Barnett et al., 2014; Tejada & Bearman, 2015). These infections are associated with long-term disability, increased length of stay, and higher risk of death (WHO, 2009). Healthcare-associated pathogens include many which can be MDROs (Centers for Disease Control, CDC, 2019; Istenes, 2011). There is limited information available to the public as states have different reporting criteria and not all states require HAI reporting (Cohen et al., 2014, National Council of State Legislatures, 2020).
Although hand hygiene is frequently mentioned to the public to address community-associated infections, the context rarely addresses the client’s role in HAI prevention Healthy People 2020, 2014; Wallace, Cropp, & Coles, 2016). Thus, it is imperative all people in all healthcare settings are vigilant regarding hand hygiene (CDC, 2016). Inadequate hand hygiene affects everyone including, but not limited to, clients, workers, visitors, family, leadership, manufacturers, and the public (Seale, et al., 2016).
The transmission of pathogens via hand contamination between healthcare workers and clients is dynamic and reciprocal, asserting the role of the client in the chain of infection and contradicting the common assumption workers are mainly responsible for transmission (Banfield & Kerr, 2005; Vaidotas et al. , 2015. There are direct consequences for the population vulnerable to HAIs (Busby et al., 2015). Several studies found clients’ hands become a reservoir and means of transmission if not adequately cleansed (Srigley et al., 2014). Healthcare reception areas have low hand hygiene adherence rates and clients’ hands may be colonized shortly after entering a healthcare setting (Vaidotas et al., 2015; Sunkesula et al., 2017).
While client hand hygiene is an obvious but frequently overlooked safety concern across healthcare settings, it is not routinely measured (Cheng et al., 2016). However, workers’ adherence to hand hygiene has recently been deemed a quality indicator with mandated public disclosure. Any publicly reported hand hygiene metric will suffer because the credibility of various methods has yet to be established, leading to distrust of the data due to misaligned incentives (Ellingson et al., 2014). For example, there is no national standard for the optimal number of hand hygiene observations or which indications should be monitored (Chassin, Mayer, & Nether, 2015a; Chassin, Nether, Mayer, & Dickerson, 2015b).
This paper presents a formal, intentional, systematic appraisal of the evidence for client hand hygiene. Evidence-based practices (EBPs) are delineated to enable facilities to discover their key causes of client hand hygiene failure and to deploy a set of customized practices to target their key causes. Interventions should be customized to specific locations and circumstances as the facility’s key causes may be the most important determinant of the intervention’s success or failure (Chassin et al., 2015a; Chassin et al., 2015b). The role and responsibilities of all within the healthcare community are addressed. Finally, we promote a multimodal strategy to address the facility’s most significant issues.
Materials/Methods of the Interventions
Hygiene and infection prevention and control strategies have traditionally been nursing responsibilities. Nurses possess the capacity to educate healthcare workers and clients about the importance of hand hygiene (Larson, 2016). Accordingly, we structured our findings to the nursing process developed in 1958 by Ida Jean Orlando to guide patient care. The five sequential steps are assessment, diagnosis, planning, implementation, and evaluation (Toney-Butler, 2019).
A literature review was conducted to assess evidence from qualitative, quantitative, and mixed methods studies. We screened for relevance by reviewing the titles and abstracts of identified papers and identified key studies pertaining to client hand hygiene. From there, we pursued references of references. We also consulted national and international infection control guidelines. We appraised the scientific literature using Dang and Dearholt’s (2018) five levels of evidence with Level 1 being the most stringent to develop and support our position on client hand hygiene (Dang & Dearholt, 2018). We included 54 studies spanning 17 years (2002-2019). We also included 31 studies published during the last 5 years in professional peer reviewed journals and 23 seminal studies more than 5 years old (Appendix A). The studies included several different countries, healthcare systems, and settings (hospitals, long-term care facilities, and the community), with hospitals being the most frequent setting. Studies differed in focus, design, and methods. Because of ethical considerations in randomizing control groups, hand hygiene research in general has lagged compared to other healthcare research topics, with few randomized trials or epidemiologically rigorous observational studies. Research around client hand hygiene is scarce and little is known about research on client hand hygiene.
Results/Data/Outcomes
Studies showed effective education increased the frequency of client hand hygiene, decreasing the pathogens found on their hands, and, subsequently, decreasing HAI rates across the healthcare settings (Cure & Van, 2015; Kundrapu et al, 2014; Pokrywka et al. , 2017). Studies have shown a correlation between the lack of worker accountability and decreased hand hygiene adherence. Therefore, it is important to provide education and training for all who work or enter the healthcare setting regardless of role (Chassin et al., 2015a). Effective education led to client and worker engagement and increased worker hand hygiene adherence (Fox et al., 2015) and increased the frequency of visitor/family hand hygiene (Sunkesula et al., 2015). Effective education of parents regarding the importance of hand hygiene increased child welfare (Bowen et al., 2012).
Home hand hygiene habits are often not applied in a healthcare setting (Barker et al., 2014). Client hand hygiene practice is affected by time of day and availability and placement of hand hygiene supplies (Ellingson et al., 2014; Hobbs et al., 2016). Issues regarding client hand hygiene adherence may include inaccessible supplies, irritating agents, lack of knowledge, forgetfulness, or lack of administrative leadership/support (O’Donnell et al., 2015). Barriers to implementing client hand hygiene programs include lack of administrative support, workload, and negative attitudes. Ineffective education may also contribute to decreased hand hygiene (Knighton et al., 2018). Factors affecting the success of the education intervention depend on clearly stated instructions and the client willingness and ability to adhere to the intervention (Chassin et al., 2015a; Chassin et al., 2015b). For example, decreased cognitive ability or motor function, and presence of orthopedic devices or bandages may interfere with their ability to perform hand hygiene (Hill et al., 2015; Burnett, Lee, & Kydd, 2008).
Recommendations
We recommend a multimodal strategy for the development of a client hand hygiene education program. First, assess the current adherence to client hand hygiene and specific potential root causes for non- adherence (Chassin et al., 2015a). Once the root causes are understood, it is important to define the barriers specific to the facility or unit (Chassin et al., 2015a; Chassin et al., 2015b). This includes identifying themes which impact hand hygiene adherence and causes of non-adherence to precisely define the problem (Chassin et al., 2015a; Chassin et al., 2015b, Morales, 2017).
Next, plan interventions directed at the facility’s unique causes of hand hygiene failure since different causes require different remedial measures. This will help invest resources where needed and avoid wasting resources on problems the facility does not have. A “one size fits all” approach does not allow for customized improvement. Attempting to address hand hygiene globally with the same plan is not likely to address problems which differ among facilities (Chassin et al., 2015a; Chassin et al., 2015b).
Important to the success of the plan is leadership engagement, which critical to facilitating a culture change (McInnes et al., 2014). Ensure facility leadership is aware and supportive of hand hygiene improvement strategies and supports these efforts with adequate resources (Chassin et al. ,2015a; Chassin et al., 2015b). Use a behavioral framework and recognized behavioral techniques to plan and execute interventions (Tuong, Larson, Armstrong, 2014). This should be a bundled plan which includes education, reminders, and feedback (Schweizer et al., 2014). We recommend the facility adopt an individualized plan, with videos, audio, and print materials to promote and sustain hand hygiene adherence (Morales, 2017, Tuong et al., 2014; Randle et al., 2014; McGuckin & Govednik, 2013). A digital support system may also promote and sustain hand hygiene adherence.
Finally, hold everyone accountable and responsible. Include hand hygiene in the clients rights and responsibilities (American Hospital Association Patient Care Partnership and on the Rights and Responsibilities of Residents of Long-Term Care Facilities) to promote high quality care, a clean and safe environment, and client involvement (Chassin et al., 2015a; Chassin et al., 2015b; Morales, 2017). Available resources and resources which can be modified to target the client are listed in Appendix B.
Once the plan is implemented, it must be sustained for long-term benefits. We recommend incorporating and maintaining the following key points for successful implementation:
- Encourage healthcare client engagement and emphasize personal responsibility and altruism (Busby et al., 2015; Cheng et al., 2016; Morales, 2017; McInnes et al., 2014). However, healthcare workers will need assist clients with hand hygiene as needed (Cheng et al., 2016; Sunkesula et al., 2015).
- Empower clients and stakeholders to have a role in HAI prevention (Seale et al., 2016; Cheng et al., 2016; McInnes et al., 2014).
- Implement plans to target specific causes and to sustain improved performance, changing reminders periodically for effectiveness (Chassin et al., 2015a; Chassin et al., 2015b).
- When designing the education plan, build on the home behaviors of the client by exploring their pre-existing attitudes and values regarding hand hygiene (Barker et al., 2014).
- Address cultural beliefs surrounding hand hygiene as it has both hygienic and ritualistic meanings. Assess and leverage the intrinsic value clients associate with hand hygiene to improve overall hospital hygiene and decrease HAIs. (Barker et al., 2014, Morales, 2017). Two available resources developed by Morales (2018) are listed in Appendix C.
Simplify education by breaking the information into components (Randle et al., 2014). Focus the education on the importance of hand hygiene and describe the available options (soap and water, alcohol-based handrubs, disposable wipes; Chassin et al., 2015a; Chassin et al., 2015b). Include the basics of infection prevention and the need for hand hygiene even if gloves or other personal protective equipment are used (Chassin et al., 2015a; Chassin et al., 2015b; Association for Professionals in Infection Control and Epidemiology [APIC], 2014). Additionally, explain the importance of avoiding touching the eyes, nose, or mouth (T-zone) to avoid self-contamination (Morales, 2017). Given the high frequency of mucosal contact, hand hygiene is essential to prevent pathogen transmission and self-inoculation (Kwok, Gralton, & McLaws, 2015).
Educational content must instruct clients on when to perform hand hygiene. There are five specific moments for client hand hygiene adapted from the World Health Organization 5 Moments of Patient Hand Hygiene (WHO, 2009; Rai et al., 2017). These are: 1) Before and after touching their wounds, devices and anything within reach, including the call button/remote, phone, service animals, etc.; 2) Before eating; 3) After using the toilet; 4) When entering or leaving the care area; and 5) In view of workers when they enter the care area which provides an unspoken reminder to workers to clean their hands before providing care. An example educational script is included in Appendix D.
Education should be provided in various forms to address limitations in literacy, physical function, or sensory perception. Education may be provided individually and/or in groups (Knighton et al., 2018; Morales, 2017; Kwok et al., 2015). Since people may often forget to perform hand hygiene, verbal and visual cues may reinforce and remind everyone thereby improving adherence (Chassin et al., 2015a; Morales, 2017). Verbal reminders can include automated audio prompts, hand hygiene champions, or reminders from workers (Morales, 2017; Rai et al., 2017; Knighton et al., 2017). Automated systems may provide real-time reminders and generate feedback for quality improvement (Chassin et al., 2015a; Chassin et al., 2015b). Champions can provide just in time coaching to encourage accountability and improve adherence. Champions can determine the cause of non-adherence and engage appropriate interventions based on the root cause (Chassin et al., 2015a). Visual reminders include stickers, posters or pamphlets focused on targeted behavior change rather than simply conveying information (Chassin et al., 2015a; Chassin et al., 2015b; Morales, 2017). Assess learning comprehension by having the learner repeat the key concepts either verbally or by demonstration.
Select appropriate hand hygiene supplies as client preference plays a role in adherence. Include several options such as soap (non-antimicrobial or antimicrobial) and water, disposable wipes, and alcohol-based handrubs when possible. Some clients find disposable wipes difficult or unpleasant to use. Others prefer push down pumps for alcohol-based handrubs (Chassin et al., 2015a; Morales, 2017; Rai et al., 2017; Knighton et al., 2017; Senol et al., 2014). Although handrubs with an alcohol concentration of 60% may decrease methicillin resistant Staphylococcus aureus colonization, incomplete removal is common (Sunkesula et al., 2015). There is a lack of evidence to support the use of triclosan containing soap compared with alcohol- based handrubs, benzalkonium chloride, or chlorhexidine gluconate (CHG: Chassin et al., 2015a; Chassin et al., 2015b; Therattil et al., 2015). While the judicious use of 2% CHG may help to prevent HAIs, chlorhexidine-free supplies may prevent allergic reactions in sensitive people (Chassin et al., 2015a; Chassin et al., 2015b).
Hand hygiene supplies must be accessible and easy to use as ineffective placement of supplies decreases hand hygiene (Ellingson et al., 2014; Hobbs et al., 2016; O’Donnell et al., 2015). Visibility and accessibility of the supplies (upon entry to the care area, on meal trays, etc.) influences adherence, therefore accommodate clients who cannot easily get to the sinks or wall-mounted dispensers (Ellingson et al., 2014; Cure et al. , 2015; O’Donnell et al. , 2015). Full hands also decrease adherence; ensure there is a convenient spot to place items and develop a maintenance plan to ensure supplies are always fully stocked (Chassin et al., 2015a).
Evaluate the intervention on a regularly scheduled basis (McInnes et al., 2014). Collect hand hygiene adherence data and report results accurately and frequently. Meaningful data includes a target and an action plan in place for improving adherence, such as unit or role-based adherence (Chassin et al., 2015a; Chassin et al., 2015b). Evaluate performance by incorporating a measurement system to audit adherence (McInnes et al., 2014). Commit to collecting and analyzing data using the same methods so the data can be compiled across sites. Avoid the use of self-report as the primary method of hand hygiene adherence. Direct observations can measure adherence as well as identify barriers to hand hygiene. Inter-rater reliability must be assured. A combination of measurement approaches is appropriate and may be adjusted for facility specific needs (Chassin et al., 2015a; Chassin et al., 2015b; Cheng et al., 2016). Most measurements of hand hygiene are for healthcare workers and usually only include entry and exit of care areas (“in and out”; Dawson & Mackrill, 2014). One easy measurement may be client hand hygiene pre-meal or upon entry and exit from the care area (Chassin et al., 2015a; Chassin et al., 2015b). An ultrasound-based location system may measure client hand hygiene in real-time during visits to the toilet, mealtimes, and on entering and leaving the care areas (Srigley et al., 2014).
Reconceptualize non-adherence and develop progressive remediation for all (Chassin et al., 2015a; McInnes et al., 2014). A robust process improvement examines the complicated problem of non-adherence and discovers highly effective, targeted interventions focused on the causes prevalent at each facility. When there is a decline in client hand hygiene, the Targeted Solution Tool provides specific recommendations to identify causes and increase adherence. Real-time displays of hand hygiene adherence may provide incentive for improvement (Chassin et al., 2015a; Chassin et al., 2015b). Consider recognition or rewards for those who model hand hygiene behaviors or improvements.
Client hand hygiene is an evidence-based strategy to reduce HAIs which are “never events” – preventable and egregious events which should never happen (Centers for Medicare and Medicaid Services, 2008). Facilities are not reimbursed for costs associated with “never events.” An increase in the perception of healthcare workers’ caring may improve client satisfaction which will also greatly impact reimbursement. Despite universal acknowledgment hand hygiene is the single most effective way to prevent the spread of pathogens, client hand hygiene is seldom addressed. We have presented several strategies to develop interventions to address these barriers which do not hinder the workflow of the worker. The evidence-based multimodal strategy presented here is affordable, practical, effective, acceptable, safe, and equitable. Additionally, policy makers should create legislation mandating facilities provide education to clients about cleaning their hands.
Acknowledgments
We would like to thank the Healthcare Infection Transmission Systems (HITS) Consortium for their support and all those who participated in the Workgroup on Hand Hygiene.
References
Association for Professionals in Infection Control and Epidemiology. (2014). Infection prevention basics. Retrieved from http://clients.site.apic.org/infection-prevention-basics/
Banfield, K. R., & Kerr, K. G. (2005). Could patients’ hands constitute a missing link? Journal of Hospital Infection, 61, 183–188.
Barker, A., Sethi, A., Shulkin, E., Caniza, R., Zerbel, S., & Safdar, N. (2014). Patients’ hand hygiene at home predicts their hand hygiene practices in the hospital. Infection Control & Hospital Epidemiology, 35, 585-588. doi: 10. 1086/675826
Barnett, A., Page, K., Campbell, M., Brain, D., Martin, E., Rashleigh-Rolls, R.,Graves, N. (2014). Changes in Healthcare-Associated Staphylococcus aureus Bloodstream Infections after the Introduction of a National Hand Hygiene Initiative. Infection Control & Hospital Epidemiology, 35(8), 1029-1036. doi:10. 1086/677160
Bowen, A., Agboatwalla, M., Luby, S., Tobery, T., Ayers, T., & Hoekstra, R. M. (2012). Association Between Intensive Handwashing Promotion and Child Development in Karachi, Pakistan: A Cluster Randomized Controlled Trial. Archives of Pediatrics & Adolescent Medicine, 166, 11, 1037.
Busby, S. R., Kennedy, B., Davis, S. C., Thompson, H. A., & Jones, J. W. (2015). Assessing patient awareness of proper hand hygiene. Nursing, 45(5), 27–30. https://doi.org/10.1097/01.NURSE.0000463667.76100.06
Burnett, E., Lee, K., & Kydd, P. (2008). Hand hygiene: What about our patients? British Journal of Infection Control, 9, 19-24.
Cao, J., Min, L., Lansing, B., Foxman, B. , & Mody, L. (2016). Multidrug-resistant organisms on patients’ hands: a missed opportunity. The Journal of the American Medical Association Internal Medicine, 176(5), 705-706.
Chassin, M. R., Mayer, C., & Nether, K. (2015a). Improving hand hygiene at eight hospitals in the United States by targeting specific causes of noncompliance. Joint Commission Journal on Quality and Patient Safety, 41, 1, 4-12.
Chassin, M. R., Nether, K., Mayer, C., & Dickerson, M. F. (2015b). Beyond the collaborative: Spreading effective improvement in hand hygiene compliance. Joint Commission Journal on Quality and Patient Safety, 41, 1, 13-25.
Cheng, V. C. C., Tai, J. W. M., Li, W. S., Chau, P. H., So, S. Y. C., Wong, L. M. W., Ching, R. H. C., Ng, M. M. L., Ho, S. K. Y., Lee, D. W. Y., Lee, W. M.,L. , Wong, C. Y. , Yuen, K. Y. (2016). Implementation of directly observed patient hand hygiene for hospitalized patients by hand hygiene ambassadors in Hong Kong. American Journal of Infection Control, 44, 6, 621-624.
Centers for Disease Control. (2019). Diseases and organisms in healthcare settings. Retrieved from http://www.cdc.gov/HAI/organisms/organisms.html#g
Centers for Disease Control. (2016). National and state healthcare-associated infections progress report. Retrieved from: http://www.cdc.gov/hai/progress-report/index.html.
Centers for Disease Control. (2015). Hand hygiene in healthcare settings. Retrieved from https://www.cdc.gov/handhygiene/patients/index.html
Centers for Disease Control. (2002). Guideline for hand hygiene in healthcare settings: Recommendations of the healthcare infection control practices advisory committee and the HICPAC/SHEA/APIC/IDSA hand hygiene task force. Retrieved from http://www.cdc.gov/mmwr/PDF/rr/rr5116.pdf
Centers for Medicare and Medicaid Services. (2008). CMS improves patient safety for Medicare and Medicaid by addressing never events. Retrieved from https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2008-Fact-sheets-items/2008-08-042.html
Cohen, C. C., Herzig, C. T. A., Carter, E. J., Pogorzelska-Maziarz, M., Larson, E. L., & Stone, P. W. (2014). State focus on health care-associated infection prevention in nursing homes. American Journal of Infection Control, 42, 4, 360-365.
Cure, L., & Van, E. R. (2015). Effect of hand sanitizer location on hand hygiene compliance. American Journal of Infection Control, 43, 9, 917-921.
Dang, D., Dearholt, S., Sigma Theta Tau International., & Johns Hopkins University. (2018). Johns Hopkins Nursing evidence-based practice: Model and guidelines. Indianapolis, IN: Sigma Theta Tau International.
Dawson, C. H., & Mackrill, J. B. (2014). Review of technologies available to improve hand hygiene compliance: Are they fit for purpose? Journal of Infection Prevention, 15, 222-228. doi:10. 1177/1757177414548695
Ellingson, K., Haas, J. P., Aiello, A. E., Kusek, L., Maragakis, L. L., Olmsted, R. N., Polgreen., P. M., Trexler, P., VanAmringe, M., Yokoe, D. S. (2014). Strategies to prevent healthcare-associated infections through hand hygiene. Infection Control & Hospital Epidemiology, 35, 937-960. doi:10. 1086/677145
Fox, C., Wavra, T., Drake, D. A., Mulligan, D., Bennett, Y. P., Nelson, C., Kirkwood, P., Jones, L., Bader, M. K. (2015). Use of a patient hand hygiene protocol to reduce hospital-acquired infections and improve nurses’ hand washing. American Journal of Critical Care, 24, 3, 216-224.
Healthy People 2020. (2014). Healthcare-associated Infections. Retrieved from https://www.healthypeople.gov/2020/topics-objectives/topic/healthcare-associated-infections
Hill, J., Hogan, T., Cameron, K., Guihan, M., Goldstein, B., Evans, M., Evans, C. (2014). Perceptions of methicillin-resistant Staphylococcus aureus and hand hygiene provider training and patient education: Results of a mixed method study of health care providers in Department of Veterans Affairs spinal cord injury and disorder units. American Journal of Infection Control, 42, 834-840. doi:10. 1016/j. ajic. 2014. 04. 026. 42
Hobbs. M. A., Robinson, S., Neyens, D. M., & Steed, C. (2016). Visitor characteristics and alcohol-based hand sanitizer dispenser locations at the hospital entrance: Effect on visitor use rates. American Journal of Infection Control, 44, 3, 258-262.
Istenes, N. A., Hazelett, S., Bingham, J. E., Kirk, J., Abell, G., & Fleming, E. (2011). Hand hygiene in healthcare: The role of the patient. American Journal of Infection Control, 9, E182 [abstract].
Knighton, S. C., Dolansky, M., Donskey, C., Warner, C., Rai, H., & Higgins, P. A. (2018). Use of a verbal electronic audio reminder with a patient hand hygiene bundle to increase independent patient hand hygiene practices of older adults in an acute care setting. American Journal of Infection Control, 46, 6, 610-616.
Knighton, S., McDowell, C., Rai, H., Higgins, P., Burant, C., & Donskey, C. J. (2017). Feasibility: An important but neglected issue in patient hand hygiene. American Journal of Infection Control, 45, 6, 626-629.
Kundrapu, S., Sunkesula, V., Jury, I., Deshpande, A., & Donskey, C. (2014). A randomized trial of soap and water hand wash versus alcohol hand rub for removal of Clostridium difficile spores from hands of patients. Infection Control & Hospital Epidemiology, 35(2), 204-206. doi:10. 1086/674859
Kwok, Y. A., Gralton, J., & McLaws, M. (2015). Face touching: A frequent habit that has implications for hand hygiene. American Journal of Infection Control, 43, 112-114. doi:10. 1016/j. ajic. 2014. 10. 015
Larson, E. (2016, April). Keynote address. 2016 national evidence-based practice conference – Changing landscapes: Contemporary issues influencing nursing care. Coralville, IA.
Massachusetts Hospital Association, (2016). Healthcare-associated Infections. Patient CareLink. Retrieved from http://patientcarelink.org/improving-patient-care/healthcare-acquired-infections-hais/
McGuckin, M., & Govednik, J. (2013). Patient empowerment and hand hygiene, 1997-2012. The Journal of Hospital Infection, 84, 3, 191-9.
McInnes, E., Phillips, R., Middleton, S., & Gould, D. (2014). A qualitative study of senior hospital managers’ views on current and innovative strategies to improve hand hygiene. BMC Infectious Diseases, 14, 1
Mody, L., Washer, L. L., Kaye, K. S., Gibson, K., Saint, S., Reyes, K., Cassone, M., Altamimi, S., Perri, M., Sax, H., Chopra, V., Zervos., M. (2019). Multidrug-resistant organisms in hospitals: What is on patient hands and in their rooms? Clinical Infectious Diseases, 69(11), 1837-1844.
Morales, K. (2017). Testing the effect of a resident-focused hand hygiene intervention in a long-term care facility: A mixed methods feasibility study. (PhD Dissertation). Retrieved from ProQuest Dissertations and Theses database. (Mercer University No. 10615469).
Morales, K. (2018). Tools for monitoring hand hygiene in a long-term care facility. Infection Control. Tips. Retrieved from https://infectioncontrol.tips/2018/11/27/tools-for-hand-hygiene-intervention-monitoring-in-a-long-term-care-facility/
National Council of State Legislatures. 2020. Methicillin-Resistant Staphylococcus aureus (MRSA) and Other Healthcare-Associated Infections. Retrieved from https://www.ncsl.org/research/health/healthcare-associated-infections-homepage.aspx#:~:text=Approximately%2027%20states%20have%20enacted,of%20the%20laws%20differs%20widely.
O’Donnell, M., Harris, T., Horn, T., Midamba, B., Primes, V., Sullivan, N., Shuler, R., Zabarsky, T. F., Deshpande, A., Sunkesula, V. C., Kundrapu, S., Donskey, C. J. (2015). Sustained increase in resident mealtime hand hygiene through an interdisciplinary intervention engaging long-term care facility residents and staff. American Journal of Infection Control, 43, 162-164. doi:10. 1016/j. ajic. 2014. 10. 018
Pokrywka, M., Buraczewski, M., Frank, D., Dixon, H., Ferrelli, J., Shutt, K., & Yassin, M. (2017). Can improving patient hand hygiene impact Clostridium difficile infection events at an academic medical center? American Journal of Infection Control, 45, 9, 959-963.
Rai, H., Knighton, S., Zabarsky, T. F., & Donskey, C. J. (2017). A randomized trial to determine the impact of a 5 moments for patient hand hygiene educational intervention on patient hand hygiene. American Journal of Infection Control, 45, 5, 551-553.
Randle., Arthur, A., Vaughan, N., Wharrad, H., & Windle, R. (2014). An observational study of hand hygiene adherence following the introduction of an education intervention. Journal of Infection Prevention, 15, 142-147.
Schweizer, M. L., Reisinger, H. S., Ohl, M., Formanek, M. B., Blevins, A., Ward, M. A., & Perencevich, E. N. (2014). Searching for an optimal hand hygiene bundle: A meta-analysis. Clinical Infectious Diseases, 58, 2, 248-259.
Seale, H., Chughtai, A. A., Kaur, R., Phillipson, L., Novytska, Y., & Travaglia, J. (2016). Empowering patients in the hospital as a new approach to reducing the burden of health care-associated infections: The attitudes of hospital health care workers. American Journal of Infection Control, 44, 3, 263-268.
Şenol, V., Ünalan, D., Soyuer, F., & Argün, M. (2014). The relationship between health promoting behaviors and quality of life in nursing home residents in Kayseri. Journal of Geriatrics. doi:10. 1155/2014/839685.
Srigley, J. A., Furness, C. D., Baker, G. R., & Gardam, M. (2014). Quantification of the Hawthorne effect in hand hygiene compliance monitoring using an electronic monitoring system: A retrospective cohort study. British Medical Journal Quality & Safety, 23, 974-980. doi:10. 1136/bmjqs-2014-003080
Sunkesula, V., Kundrapu, S., Macinga, D. R., & Donskey, C. J. (2015). Efficacy of alcohol gel for removal of methicillin-resistant Staphylococcus aureus from hands of colonized patients. Infection Control and Hospital Epidemiology, 36(2), 229– 231. https://doi.org/10.1017/ice.2014.34
Sunkesula, V., Knighton, S., Zabarsky, T., Kundrapu, S., Higgins, P., & Donskey, C. (2015). Four moments for patient hand hygiene: A patient-centered, provider-facilitated model to improve patient hand hygiene. Infection Control & Hospital Epidemiology, 36(8), 986-989. doi:10. 1017/ice. 2015. 78
Sunkesula, V. C. K., Kundrapu, S., Knighton, S., Cadnum, J. L., & Donskey, C. J. (2017). A randomized trial to determine the impact of an educational patient hand-hygiene intervention on contamination of hospitalized patient’s hands with healthcare-associated pathogens. Infection Control and Hospital Epidemiology, 38, 5, 595-597.
Tejada, C. J., & Bearman, G. (2015). Hand hygiene compliance monitoring: the state of the art. Current Infectious Disease Reports, 17(4), 470.
Therattil, P. J., Yueh, J. H., Kordahi, A. M., Cherla, D. V., Lee, E. S., & Granick, M. S. (2015). Randomized controlled trial of antiseptic hand hygiene methods in an outpatient surgery clinic. Wounds, 27, 347–353.
Toney-Butler, T. J., & Thayer J. M. (2019). Nursing Process. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK499937/
Tuong, W., Larsen, E. R., & Armstrong, A. W. (2014). Videos to influence: A systematic review of effectiveness of video-based education in modifying health behaviors. Journal of Behavioral Medicine, 37, 2, 218-233.
Vaidotas, M., Yokota, P. K., Marra, A. R., Camargo, T. Z., Victor, E., Gysi, D. M., Leal, F., Santos, O. F., Edmond, M. B. (2015). Measuring hand hygiene compliance rates at hospital entrances. American Journal of Infection Control, 43, 7, 694-696.
Wallace, N., Cropp, B., & Coles, J. (2016). Insurance companies pay the price for HAIs. Retrieved from https://thehcbiz.com/losing-battle-hospital-acquired-infections-hcbiz-22/
World Health Organization. (2009). WHO Guidelines for hand hygiene in health care. Retrieved from http://whqlibdoc.who.int/publications/2009/9789241597906eng.pdf
Appendix A:
Levels of Evidence Based on Dang and Dearholt (2018)
Appendix B:
Available Resources
Available resources for client hand hygiene include:
Clean Hand Count for Patients*
https://www.cdc.gov/handhygiene/patients/index.html
Available resources which could be modified for client hand hygiene include:
The Joint Commission Center for Transforming Healthcare
https://www.centerfortransforminghealthcare.org/en/
Robust Process Improvement
https://www.centerfortransforminghealthcare.org/what-we-offer/high-reliability-training/
Targeted Solution Tool
https://www.centerfortransforminghealthcare.org/en/what-we-offer/targeted-solutions-tool/hand-hygiene-tst/
Healthcare Improvement’s How to Guide
http://www.ihi.org/resources/pages/tools/howtoguideimprovinghandhygiene.aspx
Patient Advocacy Materials
https://www.cdc.gov/handhygiene/patients/index.html
WHO Observation Forms
https://www.who.int/gpsc/5may/Observation_Form.doc
WHO Self-Assessment Framework https://www.who.int/gpsc/country_work/hhsa_framework_October_2010.pdf
iScrub Application
https://apps.apple.com/us/app/iscrub-lite/id329764570
* Centers for Disease Control. (2015). Hand hygiene in healthcare settings. Retrieved from https: //www. cdc. gov/handhygiene/patients/index. html.
Appendix C:
Tools to Assess Clients Hand Hygiene Values and Beliefs
Health Beliefs Related to Hand Hygiene Tool*
Participant’s Reaction to Hand Hygiene Intervention Questionnaire **
* Morales, K. (2018). Tools for monitoring hand hygiene in a long-term care facility. InfectionControl.tips. Retrieved from https://infectioncontrol.tips/2018/11/27/tools-for-hand-hygiene-intervention-monitoring-in-a-long-term-care-facility/
Appendix D:
Sample Educational Content
What can you do to prevent healthcare-associated infections? The good news is there are simple steps you can take to prevent infections. Clean your hands regularly, especially at these important times:
- Whenever you enter or leave the care area
- Whenever hands look or feel unclean
- Whenever there is a concern if hands are clean
- Before you eat or drink
- Before touching any broken skin or before any medical procedure
- Before contact with indwelling medical devices, such as tubes to drain your bladder or administer intravenous fluids
- Before and after touching others
- After using the toilet
- After coughing or sneezing
To help prevent infecting yourself, avoid touching your eyes, nose, or mouth and always cough or sneeze into your elbow.
Ask each day if you still need any indwelling medical devices, such as tubes to drain your bladder or administer intravenous fluids. Also, ask about vaccines you need to stay healthy. While infections can be serious, taking these simple steps to prevent infection can help you take charge of your health.[1]
[1] Massachusetts Hospital Association, (2016). Healthcare-associated Infections. Patient CareLink. Retrieved from http://patientcarelink.org/improving-patient-care/healthcare-acquired-infections-hais/







